 Your new post is loading...
Your new post is loading...

|
Scooped by
Gilbert C FAURE
December 2, 2013 9:13 AM
|
A topic dedicated to allergy
ouvert dans le contexte du DESC d'Immunologie clinique et allergologie en France opened for 10 years, > 2800 Highly selected scoops in an evolving and controversial field >14.4 K Views by > 4.4 K viewers
|
|
Scooped by
Gilbert C FAURE
October 2, 2:39 AM
|
✨One of the most appreciated/liked articles in the social media of Allergy published in 2025:
Hypereosinophilia and Hypereosinophilic Syndromes: First Findings From a Nationwide Multicenter Cohort. Corresponding author: Guillaume Lefèvre
Read the article here: doi.org/10.1111/all.16463
The COHESion study is the first prospective large-scale multicenter study dedicated to all hypereosinophilia/hypereosinophilic syndrome (HE/HES) subtypes. The final diagnoses were idiopathic HES (HES-I, 47%), HE/HES-reactive (16%), HE-uncertain significance (15%), HE/HES-neoplastic (7%), HE/HES-lymphocytic (6%), IgG4-related disease (2%), and antineutrophil cytoplasmic antibody-negative eosinophilic granulomatosis with polyangiitis (EGPA) (7%). Considering all HES subtypes, the most frequent symptoms were cutaneous, respiratory and digestive symptoms (42%, 30% and 25%, respectively) followed by cardiac manifestations, vascular manifestations and ear, nose, throat (ENT) symptoms (12%, 9% and 7%, respectively).
#Allergy_journal
Read more articles published in #Allergy on clinical immunology here: https://lnkd.in/ex3Y69tY
|
|
Scooped by
Gilbert C FAURE
October 1, 10:11 AM
|
The tick-borne allergy to animal products is on the move north and west from the Mid-Atlantic and Southern states.
|
|
Scooped by
Gilbert C FAURE
September 15, 3:57 AM
|
https://lnkd.in/eF54n794 Intelligence artificielle et allergologie : où en est on? (Pour les Parisiens je fais demain soir une intervention sur le sujet avec Paris-Allergie merci à Marmouz Farid Christian MARTENS
|
|
Scooped by
Gilbert C FAURE
August 28, 2:36 PM
|
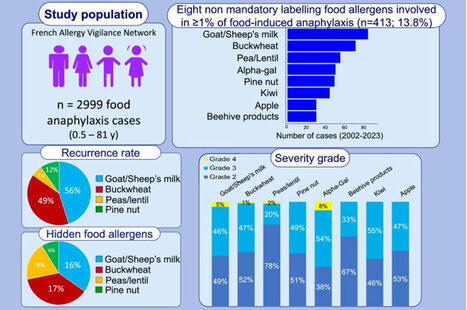
#allergies Le réseau d'allergovigilance souhaite rendre obligatoire, en Europe, la déclaration de quatre allergènes alimentaires émergents supplémentaires, sur la base d'une étude rapportée dans APMnews en décembre 2023, publiée dans Clinical & Experimental Allergy
https://lnkd.in/erY6v8_M?
|
|
Scooped by
Gilbert C FAURE
August 9, 1:37 PM
|
|
|
Scooped by
Gilbert C FAURE
August 7, 3:35 AM
|
"A blog about allergy, asthma & immunology"
|
|
Scooped by
Gilbert C FAURE
July 30, 4:30 AM
|
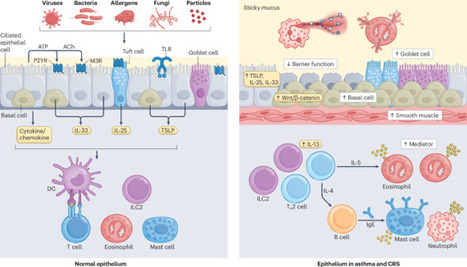
Asthma and chronic rhinosinusitis (CRS) are common chronic inflammatory diseases of the respiratory tract that have increased in prevalence over the past five decades. The clinical relationship between asthma and CRS has been well recognized, suggesting a common pathogenesis between these diseases. Both diseases are driven by complex airway epithelial cell and immune cell interactions that occur in response to environmental triggers such as allergens, microorganisms and irritants. Advances, including a growing understanding of the biology of the cells involved in the disease, the application of multiomics technologies and the performance of large-scale clinical studies, have led to a better understanding of the pathophysiology and heterogeneity of asthma and CRS. This research has promoted the concept that these diseases consist of several endotypes, in which airway epithelial cells, innate lymphoid cells, T cells, B cells, granulocytes and their mediators are distinctly involved in the immunopathology. Identification of the disease heterogeneity and immunological markers has also greatly improved the protocols for biologic therapies and the clinical outcomes in certain subsets of patients. However, many clinical and research questions remain. In this Review, we discuss recent advances in characterizing the immunological mechanisms of asthma and CRS, with a focus on the main cell types and molecules involved in these diseases. In this Review, Kato and Kita discuss the complex interactions between airway epithelial cells and immune cells that contribute to the development of asthma and chronic rhinosinusitis. They highlight recent advances in understanding the clinical heterogeneity of these diseases and explain the progress that has been made in developing new therapies.
|
|
Scooped by
Gilbert C FAURE
July 19, 8:06 AM
|
|
|
Scooped by
Gilbert C FAURE
July 8, 8:34 AM
|
8th July is World Allergy Day.
This article in Times Of India mentioned about our old study: Allergic diseases have significant impact on the quality-of-life, social life, and economy. Inadequate knowledge about allergic testing further add on to the burden of the disease. Reposting this for awareness about harmonisation of allergens testing.
The clinical suspicion of allergic sensitization can be confirmed by demonstrating the presence of allergen specific immunoglobulin-E (IgE) antibodies in vivo (skin prick test) or in vitro methods (Blood tests: FEIA, ELISA, CRD etc). There is a lack of well-defined protocols and guidelines for the diagnosis of respiratory allergy testing in India. Therefore, the evidence-based guidelines is the need of the hour.
|
|
Scooped by
Gilbert C FAURE
June 23, 6:49 AM
|
|
|
Scooped by
Gilbert C FAURE
May 28, 10:55 AM
|
#Allergie #BilanBiologique
Avec 33 % d’allergiques pour un peu plus de 1 000 allergologues en France, les délais de rendez-vous s’allongent. Les MG doivent alors assurer la prise en charge en attendant le bilan complet chez le spécialiste (tests cutanés, de provocation orale…). Faisons le point sur les bonnes pratiques en termes de bilan biologique, d’après les recos de la Société française d’allergologie.
👇👇
https://lnkd.in/gfcHxzaB
|
|
Scooped by
Gilbert C FAURE
May 16, 2:00 PM
|
Allergies : les différences d’incidences entre la ville et la campagne expliquées
|
|
|
Scooped by
Gilbert C FAURE
October 2, 2:42 AM
|
✨✨✨ Nous sommes très heureux d’annoncer la publication des résultats de #AllergenChipChallenge dans la prestigieuse revue Journal of Allergy and Clinical Immunology https://lnkd.in/e_Mn4c73
Ce projet est le fruit d’un travail collectif remarquable, qui a rassemblé cliniciens, biologistes, data scientists et chercheurs autour d’un objectif commun : mieux comprendre et interpréter les données issues des puces à allergènes et de générer par #MachineLearning un #algorithme de prédiction des #allergies à partir d'un profil d'IgE et de données cliniques.
La base de données et l'algorithme sont en libre accès au bénéfice de la recherche et des patients allergiques.
Un grand merci 🙏 à Joana Vitte et Pascal Demoly pour avoir initié ce passionnant projet, la Société Française d'Allergologie - SFA, AllergoBioNet, Health Data Hub et Bpifrance pour leur soutien déterminant, ainsi qu’à toutes celles et ceux qui ont contribué à rendre cette aventure possible Guillaume Martinroche Amir Guemari Pol André APOIL Isabella Annesi-Maesano Eric Fromentin @Laurent Guilleminault Davide Caimmi Caroline Klingebiel @Céline Beauvillain Alain Didier Jeremy Corriger Lauriane Armand Agathe Delaune Trustii.io Naama BAK CHU de Bordeaux.
➡️ Ces avancées montrent la puissance de la collaboration et de l’ouverture des données pour faire progresser la recherche en allergologie et au-delà. Le projet continue.
#OpenData #Database #Allergie #Allergologie #Allergy #Immunologie #Recherche #IA #MachineLearning #SFA #GTESIA
|
|
Scooped by
Gilbert C FAURE
October 1, 10:12 AM
|
The report updates the AAP’s 2010 guidance and emphasizes a proactive role for pediatricians in collaborating to manage student food allergies.
|
|
Scooped by
Gilbert C FAURE
September 27, 5:56 AM
|
➡️ Le CNPA a finalisé l’actualisation du Référentiel Métier d’Allergologue.
Ce travail initié sous la présidence du Dr Sébastien LEFEVRE précise les compétences et missions de l’allergologue, sa place dans le parcours de soins du patient, ses liens avec les autres spécialités et professionnels de santé.
✅ L’Allergologie se structure pour répondre aux enjeux actuels, en particulier l’augmentation de la prévalence et de la sévérité des allergies.
Ce document témoigne de l’expertise médicale et de l’engagement de notre spécialité.
Merci à toute l'équipe de rédacteurs coordonnée par LEZMI Guillaume et celle des relecteurs coordonnée par Edouard Sève.
Bonne lecture !
|
|
Scooped by
Gilbert C FAURE
August 31, 9:17 AM
|
Glad to have contributed to this international 🌎🌍🌏effort to update the #Classification and #Diagnosis of #NSAIDs 💊 #Hypersensitivity
Available: https://lnkd.in/gWQtqFAN

|
Suggested by
LIGHTING
August 11, 4:46 AM
|
Aujourd’hui, je vais vous parler de la rhinite allergique.
« Non mais arrête, il a juste un rhume ! ». C’est vrai que cela peut paraître banal, sans intérêt, même les médecins ont tendance à banaliser le « rhume ». Un nez qui coule, un nez bouché, des éternuements ? Rien de bien méchant…ça encombre les consultations des médecins traitants qui ne savent souvent pas quoi en faire… Et pourtant…nombre de ces « rhumes » sont en réalité des rhinites allergiques et les négliger ce n’est pas vous (…) , actualités des allergies : publications scientifiques lues et analysées pour vous, annonce et compte-rendus d'événements sur les allergies.
|
|
Scooped by
Gilbert C FAURE
August 8, 10:03 AM
|
|
|
Scooped by
Gilbert C FAURE
August 1, 3:34 AM
|
Nous avons uni notre expertise à celle de la SFAR pour co-construire un référentiel commun dédié au diagnostic et à la prise en charge des réactions d’hypersensibilité immédiate (HSI) en contexte périopératoire.
Découvrez quelques messages clés ci-dessous ou accédez à la ressource ici : https://lnkd.in/eKmfa9sj
|
|
Scooped by
Gilbert C FAURE
July 28, 9:48 AM
|
Have you already thought about how #terminology can influence #practice and #epidemiology? Here is a publication in #JAHD ❣️as a good example
#OccupationalHypersensitivity #HypersensitivityPneumonitis 🐦🐦⬛
|
|
Scooped by
Gilbert C FAURE
July 15, 10:42 AM
|
🚨 La T2A (Tarification à l’activité) a profondément transformé notre système de santé, mais pas toujours pour le mieux.
Résultat ? Des services d’urgence surchargés, souvent mobilisés pour des cas bénins ou des demandes sociales, faute d’outils accessibles pour comprendre les symptômes en amont.
Chez BrightNTech.AI, nous pensons qu’il est urgent d’outiller la population générale avec des assistants éthiques, capables de décoder les signaux du corps et de réorienter intelligemment vers le bon niveau de soins.
💡 C’est le rôle d’AllergIA™, notre assistant IA spécialisé en allergologie et immunologie :
✅ Analyse interactive des symptômes
✅ Aide à différencier allergies, intolérances, et autres causes
✅ Préparation d’un résumé structuré pour le pharmacien ou médecin
✅ Surtout : ne remplace jamais le diagnostic médical mais facilite un accès éclairé aux soins
📍 Ne pas saturer les urgences pour une “bobologie” n’est pas un jugement. C’est une urgence systémique. Il faut des ponts intelligents entre la technologie, le soin, et les citoyens.
👉 Découvrez #AllergIA™ ici :
https://lnkd.in/eXy5FGZ7
🔐 Développé dans le respect strict du RGPD, de l’éthique médicale et des normes européennes (MDR Class I - non diagnostic).
📋 En savoir plus sur notre approche de conformité et de santé publique : BrightNTech.AI
|
|
Scooped by
Gilbert C FAURE
July 7, 5:48 AM
|
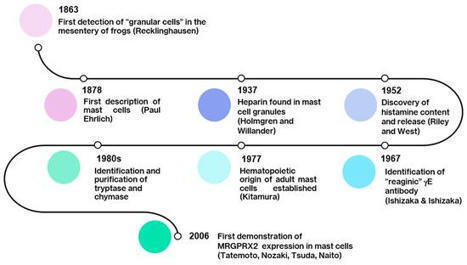
🔬 Et si on arrêtait de réduire les mastocytes à l’IgE ?
Pendant des décennies, la triade « mastocyte - IgE - allergie » a structuré notre compréhension des réactions d’hypersensibilité immédiate.
Mais aujourd’hui, nous savons que cette vision est incomplète.
📌 L’article-clé paru en janvier 2025 (Int J Mol Sci. 26(3):927) montre que les mastocytes (MC) disposent d’un répertoire de récepteurs bien plus vaste que FcεRI, et que leur activation peut suivre des voies non-IgE, dites "pseudoallergiques", via des récepteurs comme MRGPRX2.
💥 Résultat ?
➡️ Des réactions cliniques rapides, sans sensibilisation préalable ni IgE spécifique détectable.
➡️ Une dégranulation induite par des médicaments (fluoroquinolones, vancomycine, morphine...), des neuropeptides (substance P), ou des stimuli physiques.
➡️ Une inflammation neurogène amplifiée par l’interaction étroite entre MC et terminaisons nerveuses périphériques.
🧠 Les implications dépassent largement le champ allergologique classique :
- Urticaire chronique, dermatite atopique, prurit rebelle
- Syndrome d’activation mastocytaire (MCAS)
- Rosacée, asthme non contrôlé, inflammation cérébrale...
💡Comprendre MRGPRX2, c’est élargir notre cadre diagnostique et thérapeutique.
👉 De nouveaux traitements ciblent déjà cette voie : antagonistes de MRGPRX2, cannabinoïdes non-psychoactifs (PEA, CBD), anticorps anti-Siglec-8...
🧬 Les mastocytes sont bien plus que des effecteurs allergiques.
Ils sont au carrefour de l’immunité, du système nerveux et des interfaces barrière.
Et si l’on actualisait nos réflexes cliniques ?
Source : https://lnkd.in/etTeyKBh
Dr Lucie WETCHOKO
|
|
Scooped by
Gilbert C FAURE
June 12, 11:14 AM
|
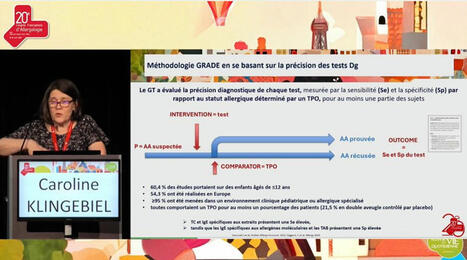
On behalf of the Allergy Diagnosis Working Group Of the French Society of Allergology (GTBA – SFA), I’m proud to have contributed to the dissemination of the EAACI guidelines on the diagnosis of IgE-mediated Food Allergy within the French-speaking medical community:
- French translation of the food allergy guidelines on diagnosis for a special issue of the French Allergy Journal (RFA) dedicated to Food Allergy: https://lnkd.in/dBAxRQXC
- Plenary presentation at the French National Congress of Allergology (CFA 2025) in Paris with a focus on methodology based on the accuracy of diagnostic tests to understand the recommended diagnostic approach: https://lnkd.in/dGAEc7PK
- Presentation at a workshop/controversy at the 30th National Congress of AMAFORCAL in Rabat, Morocco
Julien Goret, Joana Vitte, Alexandra Santos, MD PhD, Société Française d'Allergologie - SFA, European Academy of Allergy and Clinical Immunology - EAACI, @GTBA, Youness EL GUEDDARI, Elleni-Sofia Vaia
|
|
Scooped by
Gilbert C FAURE
May 24, 2:13 AM
|
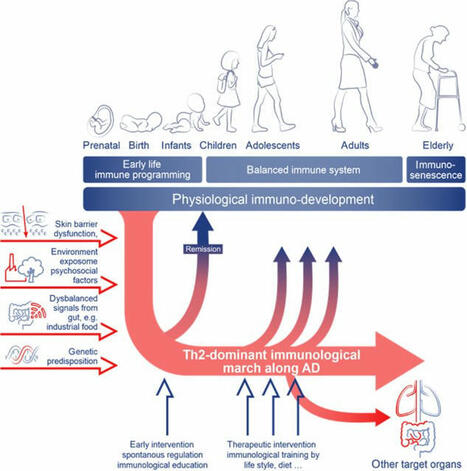
📢 One of the most appreciated/liked articles in the social media of Allergy published in 2024:
Open Access: Navigating the evolving landscape of atopic dermatitis: Challenges and future opportunities: The 4th Davos declaration. Claudia Traidl-Hoffmann
Read the article here: doi.org/10.1111/all.16247
With over 170 references and 6 figures, this article summarizes the key points discussed during the Global Allergy Forum in Davos. During this event, scientific experts and stakeholders met to address the increasing prevalence of #atopicdermatitis (AD). Topics covered include: #epithelialbarrier maintenance and disturbances in atopic diseases; #environmental changes as a driving force of atopic diseases; immunological march along the course of AD; neuroimmunology, systemic inflammation and comorbidities; therapeutic, educational, and global economic aspects; future directions
Read more articles published in #Allergy on #asthma here: https://lnkd.in/dvHaYziZ
#Allergy_journal
|
|
Scooped by
Gilbert C FAURE
May 11, 3:46 AM
|
The best critical care literature, updated daily - CCR Journal Watch
|

























2008