

Via LaLIST


|
Scooped by
Gilbert C FAURE
from LaLIST Veille Inist-CNRS
onto CME-CPD October 4, 2013 8:36 AM
|


 Your new post is loading...
Your new post is loading... Your new post is loading...
Your new post is loading...
|
|
|
Scooped by
Gilbert C FAURE
April 7, 1:46 PM
|


Certification périodique : ce que les responsables formation des établissements de santé doivent savoir maintenant
Les 52 référentiels de certification périodique sont publiés depuis le 26 février 2026. 1 438 pages couvrant les 7 professions de santé à ordre.
Voici les informations clés à retenir pour votre établissement :
Le téléservice national Ma Certif'Pro Santé ouvrira en novembre 2026.
Développé par l'Agence du Numérique en Santé, il permettra à chaque professionnel de suivre son parcours de certification sur les 4 axes réglementaires.
Les employeurs disposeront d'un accès dédié au téléservice pour suivre leurs professionnels salariés, conformément au décret n° 2025-1335. Cet accès permettra notamment d'être alerté lorsqu'un professionnel est identifié en risque de non-réalisation de son programme.
L'automatisation sera progressive. En V1, seules les attestations de l'ANDPC, de l'ANFH et de la HAS seront remontées automatiquement. Pour les formations réalisées via d'autres organismes ou en interne, vos professionnels devront saisir manuellement leurs actions. L'ouverture à d'autres fournisseurs est prévue en V2, après 2027.
En attendant, vos professionnels doivent conserver toutes leurs attestations pour les actions réalisées depuis janvier 2023, date d'entrée en vigueur de l'obligation.
Ce qu'il faut anticiper dès maintenant en tant que responsable formation :
→ Recenser vos professionnels à ordre par profession et spécialité → Vérifier que les attestations des actions déjà réalisées depuis 2023 sont bien archivées → Planifier les actions restantes pour que chacun valide ses 8 actions minimum sur les 4 axes → Préparer votre organisation à la coordination employeur prévue par l'article L.4022-2
Le premier cycle est de 9 ans pour les professionnels en exercice en 2023. Le compteur tourne déjà.
Sources : Décret n° 2025-1335 du 26/12/2025 · Arrêté du 26/02/2026 · Art. L.4022-2 CSP · DGOS
#CertificationPériodique #FormationSanté #Établissements #ProfessionnelsDeSanté #RH #ResponsableFormation
|
|
Scooped by
Gilbert C FAURE
April 6, 11:29 AM
|

We recently launched our new brand. While our look has changed, our purpose remains the same.
👋Allow us to re-introduce ourselves.
We are AMEE. We were born in Europe over 50 years ago and are dedicated to advancing scholarship and strengthening education across the health professions.
Our mission is to champion excellence, inspire collaboration, and support scholarship across the full continuum of Health Professions Education.
Our new brand colours are reflective of what we aspire to be as an organisation: bold, modern and confident.
Explore our refreshed identity on the AMEE website and learn more about our mission: https://ow.ly/FKJR50YBPCn
#AMEE #Design #Brand #HealthProfessionsEducation #HPE #Education #Scholarship
|
|
Scooped by
Gilbert C FAURE
April 2, 1:57 PM
|

Background: Artificial intelligence (AI) is increasingly integrated into education and health care, raising questions about how students use these technologies and how AI influences their learning. In health education, understanding these trends is particularly important because student learning...
|
|
Scooped by
Gilbert C FAURE
March 31, 11:08 AM
|
🎉 AMEE has a brand new look!
Health Professions Education is changing, and so are we.
Our updated branding reflects the vibrant, global community AMEE has become over the last 50+ years, a place where educators at every stage can connect, grow and inspire.
We may look different, but our mission stays the same: supporting you, supporting each other, and advancing Health Professions Education worldwide.
|
|
Scooped by
Gilbert C FAURE
from Hésitations Vaccinales: Observatoire HESIVAXs
March 29, 4:03 AM
|

Close to 1,000 health care professionals have registered for our (FREE) CME Module, and the rave reviews keep pouring in:
➡️ "This program is a game-changer for anyone working in patient care."
➡️ "It’s wonderful. Very well prepared in very simple language."
➡️ "A great education program. I've already shared it with my colleagues."
The module, worth 1.0 CME credits, includes four discreet micro-lessons:
1. Taking AIMS: How to Handle, and Overcome, Patient Resistance
2. The Power of Presumptive Recommendations
3. HCPs as Trusted Messengers
4. How to Answer Any Question
Tools, tactics, and strategies you need to sharpen your communication skills and strengthen your status as a trusted messenger.
For more info and/or to register: https://lnkd.in/eHYxFSiM
|
|
Scooped by
Gilbert C FAURE
March 24, 8:05 AM
|

🔜 EACCME Sessions at the UEMS Congress 2026‼️
The UEMS Congress is approaching, and EACCME is preparing two pivotal sessions that look ahead to the future of CME/CPD — a future shaped by innovation, complexity, and evolving educational needs:
🔎 The Core Challenges for the Accreditation of CME/CPD in the Future (2030–2050)
🔎 Defining and assessing learning needs
📍 Friday 29th May | Leuven
🚀 Key topics include:
- AI in CME: opportunity and new quality standards
- Accrediting simulations & immersive learning
- The hybrid zone: education vs. clinical decision support
- Quality over quantity: redefining meaningful CME
- Independence & integrity in 2030+
- Workforce strain & information overload
- Needs assessment
- Relevance to accreditation: what should accrediting bodies and providers change by 2030?
Join us in Leuven to reflect on how accreditation must evolve to ensure relevance, credibility, and educational impact for tomorrow’s healthcare professionals.
✨ Looking forward to seeing you there!
#UEMS #UEMSCongress2026 #EACCME #UEMSfuture
|
|
Scooped by
Gilbert C FAURE
March 7, 9:29 AM
|

Certification périodique des professions de santé : publication des référentiels.
Plus de 50 référentiels sont désormais publiés, précisant les actions permettant aux professionnels de répondre à leur obligation de certification périodique. Élaborés par les Conseils nationaux professionnels en lien avec la Haute Autorité de santé (HAS), ces référentiels structurent les démarches autour de quatre axes :
✔ actualisation des connaissances et compétences
✔ amélioration de la qualité et de la sécurité des pratiques
✔ relation avec les patients
✔ santé du professionnel
Ces référentiels constituent un cadre de référence pour accompagner le développement professionnel tout au long de la carrière.
|
|
Scooped by
Gilbert C FAURE
February 24, 4:03 AM
|

Un nouveau décret pour accompagner la qualité des soins.
A partir de 2026 les actions DPC font partie du parcours de certification de chaque médecin. L’obligation triennale de DPC disparait.
|
|
Scooped by
Gilbert C FAURE
February 21, 5:43 AM
|

It was a great week of learning and networking. Delighted to make up the majority of the record number of European participants attending the annual meeting of the Alliance For Continuing Education in the Health Professions.
Also a privilege to lead our session on cultural and generational considerations in European and global CME/CPD.
Celeste Kolanko, Emily Harrison, Monica Ghidinelli, Eugene Pozniak, Caitriona Forde, Katie Eustace, Elsbeth Headley and Caroline Halford
#Alliance2026 #cmecpd #meded #europeanCME
|
|
Scooped by
Gilbert C FAURE
January 15, 4:22 AM
|
Je participe à l’événement “17th McMaster University Review Course in Internal Medicine”. Rejoignez-moi le 22 janvier.
Cela peut intéresser les Médecins Polyvalents/ Médecins Internistes Généraux Hospitaliers !
Société Française de Médecine Polyvalente SFMP
Commission Jeunes Praticiens (CJP) de la SFMP
|
|
Scooped by
Gilbert C FAURE
January 8, 7:38 AM
|
📣 7 janvier 2026 marque une étape majeure pour l’IA en santé.
OpenAI lance ChatGPT Santé, une expérience inédite qui permet de connecter vos données personnelles de santé pour obtenir des réponses contextualisées et utiles à vos questions santé — sans diagnostic médical.
🔍 Pourquoi c’est important ?
➡️ Répondre à une demande massive d’informations santé
➡️ Contextualiser les données personnelles (Apple Health, dossiers médicaux, etc.)
➡️ Repousser les frontières entre technologie, médecine et régulation
🌍 Et pendant ce temps en Europe ?
Alors que l’accès est pour l’instant limité hors UE, des acteurs comme Doctolib développent des assistants IA patients conformes aux normes européennes — une réponse souveraine à ces nouveaux enjeux.
📯 Newsletter complète ➜ enjeux, régulation, risques, opportunités et comparatif USA vs Europe.
Ce post appartient à l’univers IAtrogénique × IAtus, mes deux IA complémentaires. Chaque réflexion possède son “double” : une version critique (IAtrogénique) et une version narrative (IAtus).
Abonnez-vous à la newsletter : https://lnkd.in/eENTNBWR
#Santé #IA #IAenSanté #ChatGPT #HealthTech #Innovation #RGPD #DonnéesDeSanté
Rémy TESTON Chanfi MAOULIDA Stéphane OHAYON Barbara Mathian Patrick Callier Stanislas Niox-Chateau Ludivine Raffin Brice Bottégal Pascal BECACHE Fabien GUEZ Bernard castells Yann-Mael Le Douarin David Sainati Hela Ghariani David Ledru Jean-Christophe Zerbini Pierre Simon Isabelle Cambreleng Antoine Tesniere Thanusian RASANAYAGAM Claire Portefaix Stéphane KIRCHE Benoit Lequeux Thierry Garban Nicolas Néaume Nadia Simon Eric Fromentin Nemanja Milenkovic Gildas AUFFRET Didier MENNECIER 🩺 Emilie Mercadal Guillaume Laguette eudes menager CEDRIC VILLEMINOT Frederic Jallat Florent Chapel Stéphane LAURENT | 16 comments on LinkedIn

|
|
Scooped by
Gilbert C FAURE
April 19, 8:01 AM
|

Expérimentation d’évaluation des actions de DPC par les professionnels de santé Ecouter À partir du 13 avril 2026, un questionnaire est adressé par l’Agence du DPC aux professionnels de santé entrant dans le périmètre de l’expérimentation, pour recueillir leur avis sur l’action de DPC à laquelle...
|
|
Scooped by
Gilbert C FAURE
from Hésitations Vaccinales: Observatoire HESIVAXs
April 7, 4:54 AM
|

Vaccine adherence: small act, global impact.
More than 150 million lives have been saved by vaccines since 1974.
Science made it possible, but it is everyday practice that sustains that impact.
At CMEPEDIA, we offer free, independent CME courses designed to support real-world clinical decision-making. Our modules on Rabies Vaccination in India and Pneumonia Vaccination in India bring together current guidelines, practical approaches, and strategies to improve vaccine adherence in everyday practice.
Every dose administered, every schedule followed, every patient conversation—these are the moments where global health outcomes are shaped.
Yet in practice, challenges persist. Vaccine hesitancy, uncertainty around eligibility, and gaps in implementation continue to affect uptake.
For healthcare professionals, staying updated is not optional. It directly influences outcomes.
Because improving adherence does not start with policy. It starts with informed care.
Create a free account on Cmepedia and start learning.
https://lnkd.in/gx9F76QD
Learn More:
https://www.cmepedia.com/
World Health Organization
#worldhealthday
|
|
Scooped by
Gilbert C FAURE
April 2, 1:57 PM
|

/PRNewswire/ -- Today, the Obesity Medicine Association (OMA) announced the launch of Treating Obesity First, a new national initiative anchored by OMAr, an...
|
|
Scooped by
Gilbert C FAURE
April 2, 1:18 PM
|
🚨📅 UEMS Congress 2026 - The final programme is now available featuring
all speakers and session abstracts ✅
🗓 Dates: 27–30 May 2026
📍 Location: UZ Leuven, Campus Gasthuisberg, Leuven (Belgium)
🌐 Register now: www.uemscongress.eu
Take a look and start planning your UEMS congress experience :
🔑 EACCME sessions with speakers representing providers, national accreditation authorities and European societies
🔑 Medical experts from UEMS and from other organisations, such as Standing Committee of European Doctors (CPME), European Union of General Practitioners, FEMS - European Federation of Salaried Doctors, or CEOM
🔑 Policy makers from the European Commission and WHO-Europe
📧 If you have any questions or need assistance with registration, please contact our Professional Congress Organiser, Nicole Elzebroek, at meetings@adevez.com.
🤝 We look forward to welcoming you to Leuven for an inspiring and engaging UEMS Congress.
#uemscongress2026 #uems #eaccme #finalprogramme #leuven
|
|
Scooped by
Gilbert C FAURE
March 31, 10:46 AM
|
📣 New podcast episode 📣
"Future-ready CPD: Balancing innovation with human connection".
On today’s episode Lisa Sullivan is in conversation with Journal of CME 2026/27 Special Collection Guest Editors Jann Balmer and Maureen Doyle-Scharff,
https://lnkd.in/ery8DFJS
The conversation explores how technology interfaces with the work of healthcare professionals. It is not just about AI, technology or innovation, but about the broader interface of all factors that go beyond just knowledge acquisition, including collaboration and team-based learning, that has an effect on clinical practice with the potential to make an impact on patient care.
More information about the 2026/27 Special Collection can be found on the journal website: jcme.org
The podcast is available as video on YouTube and Spotify, and audio on all other platforms.
#cmecpd #meded #19ECF
|
|
Scooped by
Gilbert C FAURE
March 24, 11:25 AM
|

A record number of Europeans were at the Alliance For Continuing Education in the Health Professions meeting in Atlanta last month... but what did they think if it and what lesson did they find valuable to apply in their European and global CME/CPD practice?
Listen in as they share their thoughts. A huge thank you to:
Sven Awege — France
Daniela Clape — Spain
Katie Eustace — Netherlands
Hannah Fisher — UK
Caitriona Forde — UK
Monica Ghidinelli — Switzerland
Christine Ghione — Spain
Caroline Halford — UK
Emily Harrison — UK
Elsbeth Headley — UK
Celeste Kolanko — UK
Dr Phil McElnay — Ireland
Eugene Pozniak — UK
Robin Stevenson — UK
Lisa Sullivan — Australia
Joel Turner — UK
Available on YouTube and Spotify as video as well all other platforms.
https://lnkd.in/eacA8YwC
#CMECPD #Alliance2026 #meded #19ECF
|
|
Scooped by
Gilbert C FAURE
March 14, 2:11 PM
|

Collaborating with Holly Harris, Charlotte Denniston, Tina Penick Brock, and Sophie Soklaridis has been such a joy.
This article was a wonderful way to reflect on what we’ve learned as we’ve been developing a values-based partnership together 😊
|
|
Scooped by
Gilbert C FAURE
March 1, 11:07 AM
|
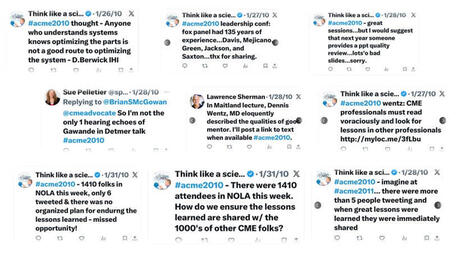
Reflecting on the first ever CME/CPD conference hashtag (#)
|
|
Scooped by
Gilbert C FAURE
February 23, 10:42 AM
|
From a distance last week (for reasons many of you know), I followed several Alliance sessions focused on global CPD. At the same time, recent conversations with both CME/IME/CPD providers and supporters working across regions have been circling around many of the same questions.
Together, they reinforced an observation that continues to surface across regions:
There is no single model of global CPD.
There are only local systems, each shaped by culture, regulation, healthcare delivery, professional expectations, and available resources. And levels of CPD Literacy vary greatly between countries and regions as well.
Across countries, CPD systems range from highly mature to still emerging, and many look very different from those we are accustomed to in the US or Europe. Yet we often approach international education as if successful models can simply be cut-and-pasted.
A few lessons that experience, and research published over the past several years in Medical Teacher, the Journal of CME, and Asia Pacific Scholar (copies available upon request 😎), continue to reinforce:
• Running a symposium at an international specialty conference in another country does not, by itself, make an organization a “global” provider.
• Accreditation cannot be assumed, and sometimes should not be the starting point (but should always be researched and considered).
• Learner needs are always local, even when challenges appear global.
• Educational formats require adaptation, not replication.
• Translation changes language, not context.
• In many regions, “providers” may not exist or function as they do in the US or Europe, and some provider types may not be recognized by some systems or by learners.
• Being accredited at home does not guarantee legitimacy elsewhere.
Perhaps the most consistent insight, emerging both from research and ongoing conversations, relates to people rather than systems.
We have a global faculty preparation gap.
Many CPD faculty are exceptional clinicians and subject matter experts but have never been trained in how professionals learn once they are in practice. At the same time, many experienced health professions educators are trained to teach students and trainees, yet have not developed competencies specific to lifelong learning in complex clinical environments. There are still many places in the world where a lecture by a subject matter expert is the only form of CPD available.
This challenge appears across systems regardless of maturity level.
Global impact rarely comes from exporting education. It comes from developing educators and designing learning that fit local realities, local partnerships, and local practice environments.
Both providers and supporters are trying to balance global ambitions with meaningful local impact. The organizations making the greatest progress tend to start with listening, humility, and local collaboration before scaling solutions.
Thinking globally matters.
Designing locally is essential.
|
|
Scooped by
Gilbert C FAURE
February 23, 3:43 AM
|

We are proud to announce the official title of our new journal:
📰 European Medical Specialist Review ✨
A sincere thank you to everyone who contributed with their ideas 🙏
Your inputs demonstrate the engagement and warm welcome for this new journal. 👩⚕️👨⚕️
The European Medical Specialist Review marks an important milestone for UEMS — a new platform for all, UEMS members and non members, to advance and trigger reflection, to influence the present and shape the future of specialist medical practice and training across Europe.
The inaugural issue will be release in connection with the 1st UEMS Congress in May 2026.
🚀 The official launch comes soon! Stay tuned for more information
|
|
Scooped by
Gilbert C FAURE
February 10, 11:19 AM
|

📘 What is an ELM Course?
An ELM Course is a structured set of related learning modules designed to provide in-depth education in a specific field.
✅ To claim CME/CPD credits, learners must complete the entire course — partial completion does not qualify.
⚠️ Once an ELM Course is accredited, its content and format are fixed for the full accreditation period.
Any changes require the submission of a new application.
🎓 ELM Courses ensure consistency, quality, and transparency in accredited medical education.
#uems #eaccme #elearning #elmcourse #eacmeaccredited
|
|
Scooped by
Gilbert C FAURE
January 13, 3:45 AM
|
📍 Last Saturday, UEMS-EACCME hosted the meeting of the UEMS Advisory Council on Continuing Medical Education (CME) in Brussels.
🤝 The Advisory Council brings together colleagues from National Accreditation Authorities (NAA), National Medical Associations (NMA), as well as UEMS Sections, European Specialty Accreditation Boards (ESABs), and other partners involved in UEMS EACCME® accreditation to exchange on current issues and shape the future development of EACCME and medical accreditation in Europe.
🔍 The main topic of the meeting was the EACCME-accredited provider status, with a presentation of the ongoing work and progress achieved so far, followed by an exchange of insights, comments, and feedback from participants.
📊 The EACCME 2025 Report was also presented, highlighting the remarkable work and commitment of the accreditation team and its partners in the field of accreditation, including reviewers and experts involved in the process.
📅 Participants were reminded of the upcoming UEMS Congress, taking place on 27–30 May 2026 in Leuven, Belgium 🇧🇪.
💬 The discussions were highly productive, generating valuable insights and further reinforcing collaboration in European medical accreditation.
#uemsadvisorycouncilmeeting #accreditedprovider #uems #eaccme
|
|
Scooped by
Gilbert C FAURE
January 8, 4:56 AM
|
Nous lançons ChatGPT Santé, une expérience dédiée qui combine de manière sécurisée vos informations de santé avec l’intelligence de ChatGPT, pour vous aider à vous sentir mieux informé, préparé pour gérer votre santé.
La santé est déjà l’un des usages les plus courants de ChatGPT, avec des centaines de millions de personnes qui posent chaque semaine des questions liées à la santé et au bien-être. ChatGPT Santé s’appuie sur les mécanismes éprouvés de confidentialité, de sécurité et de gestion des données de ChatGPT, avec des protections supplémentaires spécifiquement pensées pour la santé, notamment un chiffrement dédié et une isolation renforcée afin de préserver la confidentialité et le cloisonnement des conversations de santé. Vous pouvez connecter en toute sécurité vos dossiers médicaux et vos applications de bien-être afin d’ancrer les conversations dans vos propres données de santé, pour obtenir des réponses plus pertinentes et plus utiles. Conçu en étroite collaboration avec des médecins, ChatGPT Santé aide les personnes à jouer un rôle plus actif dans la compréhension et la gestion de leur santé et de leur bien-être, tout en venant en soutien — et non en remplacement — des soins prodigués par des professionnels de santé.
le 7 janvier 2026
liste d'attente





from open access to predatory journals... but obviously a publisher is not a publisher is not a publisher!
every reader should keep an open mind to criticism
every author should maintain a tenacious search of journals
and every so-called evaluator train in scientific information!
but....