Your new post is loading...
Your new post is loading...

|
Scooped by
Gilbert C FAURE
October 12, 2022 10:22 AM
|
During the period of March 2019 to February 2021, we enrolled 36 BCG-vaccinated healthy adults between 18 and 55 years of age at McMaster University Medical Centre. Four participants were excluded (2 withdrew consent and 2 were withdrawn before vaccination because they were unable to comply with the study visit requirements) and 1 did not complete any follow-up visits after vaccination because of COVID restrictions. Thirty-one participants completed the study: 11 in the low-dose (LD) aerosol group, 11 in the high-dose (HD) aerosol group, and 9 in the i.m. group (Figure 1). The demographic and baseline characteristics of the study participants were similar among study groups (Table 1). Figure 1Trial profile. PPD, purified protein derivative; LD, low-dose aerosol; HD, high-dose aerosol; i.m.-intramuscular injection; PFU, plaque-forming unit. Table 1Demographics of participants. Characterization of inhaled aerosol delivery method and aerosol droplets using Aeroneb Solo device. The Aeroneb Solo Micropump was selected to be part of the device set up for aerosol generation and delivery in our study (Supplemental Figure 1; supplemental material available online with this article; https://doi.org/10.1172/jci.insight.155655DS1). A fill volume (FV) of 0.5 mL in the nebulizer was determined to be optimal for vaccine delivery in saline. Subjects completed inhalation of this volume containing the vaccine via tidal breathing in approximately 2.5 minutes (Table 2). The emitted dose (ED) of vaccine available at the mouth was found to be approximately 50% of the loaded dose in the nebulizer (Table 2). The majority of aerosol droplets containing the vaccine were < 5.39 μm (85%), or between 2.08 and 5.39 μm in diameter, conducive to vaccine deposition in major airways. Thus, the amount of aerosol available at the mouth and subsequently deposited in the lung was 42.5% (16). The estimated rate of viable vaccine from aerosol droplets generated by the nebulizer was 17.4%. The dose loaded in the nebulizer for aerosol inhalation was, thus, corrected according to the estimated losses of vaccine within the device. Table 2Characterization of aerosol device and aerosol droplets. Safety of inhaled aerosol and i.m.-injected AdHu5Ag85A vaccine. Both LD (1 × 106 PFU) and HD (2 × 106 PFU) of AdHu5Ag85A administered by aerosol inhalation or the i.m. injection were safe and well tolerated. Respiratory adverse events were infrequent, mild, transient, and similar among groups (Table 3). I.m. injection was associated with a mild local injection site reaction in 2 participants. Systemic adverse events were also infrequent, mild, transient, and similar among groups (Table 3). One participant who received LD aerosol vaccine developed genital lesions consistent with primary HSV-1 infection the day following the week-2 bronchoscopy, and this condition resolved without complication with oral valacyclovir; one participant developed plantar fasciitis on day 13 following vaccination, which was attributed to mechanical strain and resolved with acetominophen. There were no grade 3 or 4 adverse events reported, nor any serious adverse events. Table 3Adverse events. There were no clinically significant abnormalities of laboratory tests at weeks 2, 4, and 12 following vaccination. Follow-up respiratory functional determinations forced expiratory volume in the first second (FEV1)and forced vital capacity (FVC) were similar to baseline values in all participants across all 3 groups (Figure 2, A and B). Figure 2Respiratory function and bronchoalveolar cellular responses following aerosol or intramuscular vaccination. (A and B) Lung function was assessed as FEV1 and FVC at baseline and 2 weeks after LD aerosol (n = 11), HD aerosol (n = 11), or i.m. (n = 9) vaccination. (C–F) Frequencies of differential cells including macrophages, lymphocytes, neutrophils, and epithelial cells in BALF from LD aerosol, HD aerosol, and i.m. vaccine cohorts. Violin plots show the median and quartiles. Data in dot plots are expressed as the mean value (horizontal line) with 95% CI. Wilcoxon matched pairs signed-rank test was used to compare various time points with baseline values within the same vaccination group. Bronchoscopy and bronchoalveolar lavage were generally well tolerated in all participants. As expected, in some participants, the procedures were associated with mild cough, sore throat, low-grade fever, headache, and a transient drop in FEV1. The appearance of the bronchial mucosa was judged as normal in all participants at each time point. Adequate bronchoalveolar lavage fluid (BALF) volumes were obtained following bronchoalveolar lavage, and on average, 10 to 20 million total cells were obtained. Aerosol AdHu5Ag85A vaccination induces robust and sustainable Th1 responses in the airway. Bronchoalveolar lavage was obtained successfully at baseline and at 2 and 8 weeks after vaccination from all participants with a median return volume of 87.5 mL (IQR, 72.5–98) from a total of 160 mL saline instilled and a median total cell number of 0.14 million/mL BALF (IQR, 0.1–0.2). Cellularity in the airway significantly increased 2 weeks after both LD and HD aerosol vaccination, and in the LD aerosol group, cellularity remained significantly heightened up to 8 weeks after vaccination compared with baseline (Figure 2C). Both LD and HD aerosol vaccination led to a transient reduction in airway macrophages, but the lymphocyte counts significantly increased only in LD cohort (Figure 2, D and E). Importantly, both neutrophils and epithelial cells in the airway remained either absent or unaltered following aerosol vaccination (Figure 2, D and E), indicating no significant airway inflammation except vaccine-induced lymphocytic responses. In comparison, there were no marked changes in total cellularity and any leukocyte subsets in the airway after i.m. vaccination (Figure 2, C and F). Evaluation of Th1 responses in the airways (BALF) cells was performed by intracellular cytokine immunostaining and flow cytometry (the gating strategy shown in Supplemental Figure 2). It showed that both LD and HD aerosol AdHu5Ag85A markedly increased Ag85A peptide pool–specific (Ag85A p. pool–specific) or reactive, IFN-γ–, TNF-α–, and/or IL-2–producing CD4+ T cells in the airways at 2 weeks after vaccination compared with the respective baseline responses (Figure 3, A–C). On average, the total Ag-specific cytokine-producing CD4+ T cells represented approximately 25% of all CD4+ T cells at 2 weeks after LD or HD aerosol, and they remained significantly elevated up to 8 weeks in the airways of LD cohort (Figure 3, A and B). In contrast, i.m. AdHu5Ag85A vaccination failed to induce Ag-specific CD4+ T cells in the airways (Figure 3A). Compared with CD4+ T cells, although the levels of airway CD8+ T cell responses were much smaller, they were significantly increased at both 2 and 8 weeks, particularly following LD aerosol vaccination (Figure 3D). Of interest, there was also a small but increased number of CD8+ T cells at 2 weeks after i.m. vaccination. Figure 3Induction of multifunctional T cells in the airways following aerosol or i.m. vaccination. (A) Frequencies of airway antigen–specific combined total-cytokine–producing CD4+ T cells at various time points in LD aerosol, HD aerosol, and i.m. cohorts. (B) Frequencies of airway single-cytokine–producing CD4+ T cells at various time points in LD aerosol cohort. (C) Frequencies of airway single-cytokine–producing CD4+ T cells at various time points in HD aerosol cohort. (D) Frequencies of airway antigen–specific combined total-cytokine–producing CD8+ T cells at various time points in LD aerosol, HD aerosol, and i.m. cohorts. (E) Representative dot plots of airways CD4+ and CD8+ T cells expressing IFN-γ, TNF-α, and IL-2 at wk2 from LD aerosol participants. (F) Frequencies of airways polyfunctional (triple/3+, double/2+, and single/1+ cytokine+) antigen-specific CD4+ and CD8+ T cells at various time points in LD aerosol group. (G) Median proportions displayed in pie chart of antigen-specific airways CD4+ and CD8+ T cells expressing a specific single or combination of 2 or 3 cytokines at various time points in LD aerosol group. Data in dot plots are expressed as the mean value (horizontal line) with 95% CI. Box plots show mean value (horizontal line) with 95% CI (whiskers), and boxes extend from the 25th to 75th percentiles. Wilcoxon matched pairs signed-rank test was used to compare various time points with baseline values within the same vaccination group. Analysis of polyfunctionality of vaccine-activated CD4+ and CD8+ T cells reactive to Ag85A in the airways revealed that LD aerosol vaccination led to induction of a higher magnitude of CD4+ T cells that coexpressed IFN-γ, TNF-α, and IL-2 (3+) and any of 2 cytokines (2+) compared with those producing single cytokine (1+) (Figure 3, E and F). Importantly, polyfunctional CD4+ T cells remained significantly increased over the baseline up to 8 weeks. Similarly, LD aerosol vaccination also significantly increased the polyfunctional CD8+ T cells, particularly at 8 weeks, in the airways, though at a much lower overall magnitude compared with CD4+ T cells (Figure 3F). In comparison, HD aerosol vaccination led to significantly increased polyfunctional CD4+ but not CD8+ T cells reactive to Ag85A (Supplemental Figure 3, A and B). Given that the LD aerosol AdHu5Ag85A was consistently highly immunogenic, we profiled the polyfunctional CD4+ and CD8+ T cells in the airways of the LD cohort in greater detail. While at 2 weeks, a greater proportion of Ag85A-reactive CD4+ T cells were polyfunctional (IFN-γ+TNF-α+IL-2+, IFN-γ+TNF-α+, or IFN-γ+IL-2+), with some of them also being single cytokine producers, at 8 weeks, the vast majority of them (>95%) became polyfunctional (Figure 3G). In comparison, most of the CD8+ T cells at 2 weeks were single-cytokine producers (TNF-α+), but at 8 weeks, the majority of them turned to be polyfunctional, mostly being IFN-γ+TNF-α+ (Figure 3G). Since the trial participants were previously BCG vaccinated, we examined the overall T cell reactivity to stimulation with multimycobacterial antigens. We found considerable CD4+ T cells present in the airways to be reactive to a cocktail of mycobacterial antigens even prior to vaccination, and they remained unaltered after LD, HD, or i.m. vaccination (Supplemental Figure 3C). These BCG-specific CD4+ T cells in the airways of LD group were mostly polyfunctional (Supplemental Figure 3, D and E). Similarly, small numbers of preexisting BCG-specific CD8+ T cells in the airways were not altered by aerosol or i.m. vaccination (Supplemental Figure 3F). The above data suggest that inhaled aerosol, but not i.m., AdHu5Ag85A vaccination can induce robust antigen-specific T cell responses within the respiratory tract. Furthermore, a LD (1 × 106 PFU) aerosol vaccination is superior to a HD (2 × 106 PFU) aerosol in inducing robust and sustainable respiratory mucosal immunity. The mucosal responses induced by AdHu5Ag85A vaccine are predominantly polyfunctional CD4+ T cells in nature, with some levels of polyfunctional CD8+ T cells. The preexisting CD4+ T cells of multimycobacterial antigen specificities in the airway of BCG-vaccinated trial participants were not significantly impacted by AdHu5Ag85A aerosol vaccination. Aerosol vaccination induces airway TRM expressing the lung-homing molecule α4β1 integrin. Lung tissue TRM are critical to protective mucosal immunity (17). Hence, we next determined whether antigen-specific T cells induced by aerosol AdHu5Ag85A vaccination were of tissue-resident memory phenotype and compared them with those induced by i.m. vaccination. BALF cells obtained before and at select time points after vaccination were stimulated with Ag85A p. pool and immunostained for coexpression of 2 key TRM surface markers CD69 and CD103 by antigen-specific IFN-γ–producing CD4+ or CD8+ T cells (Figure 4A). Marked increases in Ag85A-specific IFN-γ+ CD4+ and CD8+ T cells coexpressing CD69 and CD103 were seen only in the airway of LD and HD aerosol vaccine groups and not in i.m. group (Figure 4, B and C). Although TRM increases at 8 weeks after aerosol vaccination, compared with the baseline, were only marginally statistically significant (95% CI) probably due to small sample sizes, remarkable proportions of Ag85A-specific CD4 T cells (~20%) and CD8+ T cells (~54%) present in the airways of aerosol vaccine groups were TRM (Figure 4D). As expected, there was no detectable antigen-specific TRM in the peripheral blood before and after vaccination. Figure 4Induction of airway tissue TRM following aerosol or i.m. vaccination. (A) Representative dot plots of airway antigen–specific CD4+ and CD8+ TRM at wk2 in LD aerosol participants. (B) Frequencies of airway antigen–specific IFN-γ+CD4+ TRM coexpressing CD69 and CD103 surface markers at various time points in LD aerosol, HD aerosol, and i.m. vaccine cohorts. (C) Frequencies of airway antigen–specific IFN-γ+CD8+ TRM coexpressing CD69 and CD103 at various time points in LD aerosol, HD aerosol, and i.m. vaccine cohorts. (D) Comparison of frequencies of airway antigen–specific CD4+ and CD8+ TRM coexpressing CD69 and CD103 at 8 weeks after LD and HD aerosol vaccination. (E) Representative dot plots of peripheral blood antigen–specific IFN-γ+CD4+ T cells expressing CD49d at wk2 from LD aerosol participants, and frequencies of circulating antigen-specific CD4+ T cells expressing CD49d at various time points in LD aerosol, HD aerosol, and i.m. vaccine cohorts. (F) Representative dot plots of airway antigen–specific IFN-γ+CD4+ T cells expressing CD49d at wk2 from LD aerosol participants, and frequencies of airway antigen–specific CD4+ T cells expressing CD49d at various time points in LD aerosol, HD aerosol, and i.m. vaccine cohorts. (G) Comparison of frequencies of airway antigen–specific IFN-γ+CD4+ T cells coexpressing CD49d at the peak time point in LD aerosol, HD aerosol, and i.m. vaccine cohorts. Data in dot plots are expressed as the mean value (horizontal line) with 95% CI. Wilcoxon matched pairs signed-rank test (B, C, E, and F) was used to compare various time points with baseline values within the same vaccination group. Mann-Whitney U test (D and G) was used when comparing between vaccination groups. We also studied T cell surface expression of α4β1 integrin (VLA-4; or CD49d for α4), known to be expressed on memory CD4+ T cells in human airways (18). Since CD49d may be involved in the homing of circulating T cells to the airway, we first examined CD49d expression on Ag85A-specific CD4+ T cells in the circulation. There were small but significantly increased frequencies of circulating CD49d-expressing IFN-γ+CD4+ T cells, particularly at 2 weeks following LD or HD aerosol vaccination (Figure 4E). In comparison, there were much greater frequencies of CD49d-expressing IFN-γ+CD4+ T cells (out of total CD4+ T cells) in the airways induced by aerosol vaccination (Figure 4F), compared with their frequencies in the circulation (Figure 4E) and in contrast with the lack of such T cells in the airways of i.m. group (Figure 4G). In fact, the majority of Ag85A-specific CD4+ T cells in the airways of LD and HD groups expressed CD49d (57% and 74%, respectively). The data indicate that aerosol AdHu5Ag85A vaccination, but not i.m. route of vaccination, is uniquely capable of inducing antigen-specific T cells in the airways endowed with respiratory mucosal homing and TRM properties. Since, besides mucosal adaptive immunity, respiratory delivery of AdHu5Ag85A vaccine in experimental animals induced a trained phenotype in airway macrophages (6, 19), we examined whether aerosol vaccination could also alter the immune property of human alveolar macrophages (AM). To this end, we elected to examine the transcriptomics of BALF cells obtained from 5 participants before (week 0 [wk0]) and after (week 8 [wk8]) LD aerosol vaccination. Before RNA isolation, the cells, upon revival from frozen stock, were enriched for AM and cultured with or without stimulation with M. tuberculosis lysates and transcriptionally profiled by RNA-Seq analysis. Principal component analysis (PCA) revealed that unstimulated and stimulated AM populations were separated away from each other (Figure 5A). We then identified the differentially expressed genes (DEGs) by comparing wk0-stimulated (Group 3–stimulated) and wk8-stimulated (Group 4–stimulated) AM with respective unstimulated AM (wk0/Group 1) and wk8/Group 2). A total of 2726 genes was differentially expressed upon stimulation in pairwise analysis, of which 1667 genes (61%) were shared between the baseline (wk0) Group 3/Group 1 and aerosol vaccine (wk8) Group 4/Group 2 (Figure 5B). As expected, the shared genes were significantly enriched in biological processes associated with immune response and regulation of cell death (Figure 5C). Furthermore, by pairwise analysis, we identified 191 and 426 genes uniquely upregulated and downregulated, respectively, in stimulated aerosol (Group 4) AM (Figure 5D). The uniquely upregulated genes in stimulated wk8 aerosol AM showed enrichment in a number of biological processes including response to anoxia (OXTR, CTGF), inflammatory response to antigenic stimuli (IL-2RA, IL-1B, IL-20RB), tyrosine phosphorylation of STAT protein (IFN-γ, F2R, OSM), regulation of IL-10 production (CD83, IRF4, IL-20RB, IDO1), response to IL-1 (RIPK2, SRC, IRAK2, IL-1R1, XYLT1, RELA), and histone demethylation (KDM6B, KDM5B, KDM1A, KDM7A, JMJD6; Figure 5E). In comparison, the uniquely downregulated genes in wk8 aerosol AM did not appear significantly enriched for any biological processes. These data suggest that LD aerosol vaccination leads to persisting transcriptional changes in airway-resident AM poised for defense responses. Figure 5Transcriptomic analysis of alveolar macrophages (AM) following LD aerosol vaccination. (A) Principal component analysis (PCA) of gene expression in AM obtained before (wk0) and after (wk8) LD aerosol vaccination cultured with (S) or without (US) stimulation. (B) Venn diagram comparing all DEGs in pairwise comparison. (C) Significantly enriched functional categories of biological processes by GO associated with DEGs shared between the baseline (wk0) Group 3/1 and aerosol vaccine (wk8) Group 4/2. (D) Venn diagram comparing up- and downregulated DEGs in pairwise comparison. Heatmap shows DEG uniquely up- and downregulated, in stimulated aerosol (Group 4) AM. (E) Significantly enriched functional categories of biological processes by GO associated with uniquely upregulated DEGs in stimulated aerosol (Group 4) AM. Statistical differences in functional categories of biological processes was performed using BINGO plugin, which uses a hypergeometric test with Benjamini-Hochberg FDR correction. Both aerosol and i.m. vaccination induce systemic Th1 responses. Assessment of overall antigen-specific reactivity of T cells in the circulation before and after vaccination by using whole blood samples incubated with Ag85A peptides indicated that both aerosol, particularly LD aerosol, and i.m. AdHu5Ag85A vaccination induced significant systemic immune responses, as shown by raised IFN-γ, TNF-α, and IL-2 levels in plasma (Figure 6, A–C). AUC analysis, which reflects the overall magnitude of responses, did not differ between LD aerosol and i.m. groups in cytokine production in response to Ag85A p. pool stimulation (IFN-γ, P = 0.0910; TNF-α, P = 0.6207; IL-2, P = 0.8703). However, i.m. vaccine–induced systemic T cell responses appeared to remain significantly increased over a longer duration (Figure 6C). In comparison, the HD aerosol group had significantly lower IFN-γ production than i.m. group (AUC compared with i.m., P = 0.0117) whereas they did not differ from each other in the production of TNF-α and IL-2 (Figure 6, B and C). Figure 6Induction of antigen-specific T cell responses in the peripheral blood following aerosol or intramuscular vaccination. (A–C) Antigen-specific cytokine production in whole blood culture at various time points after LD aerosol, HD aerosol, and i.m. vaccine groups. The measurements were subtracted from unstimulated control values. (D) Frequencies of peripheral blood antigen–specific combined total-cytokine-producing CD4+ T cells at various time points in LD aerosol, HD aerosol, and i.m. cohorts. (E) Frequencies of peripheral blood polyfunctional (triple/3+, double/2+, and single/1+ cytokine+) antigen-specific CD4+ T cells at various time points in LD aerosol, HD aerosol, and i.m. vaccine groups. (F) Frequencies of peripheral blood antigen–specific combined total-cytokine–producing CD8+ T cells at various time points in LD aerosol, HD aerosol, and i.m. groups. (G) Frequencies of peripheral blood polyfunctional (triple/3+, double/2+ and single/1+ cytokine+) antigen-specific CD8+ T cells at various time points in LD aerosol, HD aerosol, and i.m. groups. Data in dot plots are expressed as the mean value (horizontal line) with 95% CI. Box plots show mean value (horizontal line) with 95% CI (whiskers), and boxes extend from the 25th to 75th percentiles. Line graphs show median with IQR. Wilcoxon matched pairs signed-rank test (A, B, E, and G) was used to compare various time points with baseline values within the same vaccination group. Mann-Whitney U test (D and F) was used when comparing vaccination groups. Further examination of relative activation of CD4+ and CD8+ T cells by aerosol and i.m. vaccinations using intracellular cytokine staining (ICS) revealed that, compared with the respective baseline, aerosol vaccination activated the circulating Ag85A-specific CD4+ T cells to significant levels, while i.m. vaccination moderately increased such responses (Figure 6D). However, the overall magnitude of responses did not differ significantly between aerosol and i.m. groups (AUC: LD aerosol, P = 0.1961; HD aerosol, P = 0.3545 compared with i.m.). Both LD/HD aerosol and i.m. vaccination also significantly increased Ag85A-specific polyfunctional CD4+ T cells coexpressing 3 (3+) or any 2 (2+) cytokines in the circulation (Figure 6E). Consistent with the airway Ag85A-specific CD4+ T cell responses (Figure 3, A–C) in both LD and HD aerosol groups, circulating polyfunctional CD4+ T cells also generally peaked at 2 weeks after vaccination and remained significantly increased up to 8 weeks (Figure 6E). In comparison, 3+ polyfunctional CD4+ T cells in the i.m. group significantly increased at 4 weeks and remained increased up to 8 weeks (Figure 6E). The overall magnitude of circulating 3+ polyfunctional CD4+ T cells in the i.m. group was, however, significantly higher than those in aerosol groups (AUC: LD aerosol, P = 0.0144; HD aerosol, P = 0.0393 compared with i.m.). Circulating 2+ polyfunctional CD4+ T cells did not differ significantly between these groups (AUC not significantly different). Consistent with our previous observation (8), besides its activating effects on circulating CD4+ T cells, i.m. vaccination also significantly increased Ag85A-specific CD8+ T cells up to 16 weeks (Figure 6F). By comparison, aerosol vaccination minimally induced such CD8+ T cells in the circulation (Figure 6F). Compared with circulating CD4+ T cells (Figure 6E), similar to the overall kinetics of total-cytokine+ CD8+ T cells (Figure 6F), circulating Ag85A-specific polyfunctional CD8+ T cells peaked behind the peak CD4+ T cell responses in all vaccine groups (Figure 6G). The kinetics of polyfunctional profiles of circulating CD4+ T cells were further examined in greater detail with a focus on the LD aerosol vaccine group and its comparison with the i.m. group. There existed considerable differences in the polyfunctional profile of circulating Ag85A-specific CD4+ T cells between LD aerosol and i.m. groups (Supplemental Figure 4A). In the LD aerosol group, the proportion of IFN-γ+TNF-α+IL-2+ progressively shrank, and at 16 weeks, approximately 75% of the population were TNF-α+IL-2+ and IFN-γ+TNF-α+ together with single TNF-α+ CD4+ T cells. In comparison, in the i.m. group, the proportion of IFN-γ+TNF-α+IL-2+ progressively expanded, constituting approximately 75% of the population at 16 weeks (Supplemental Figure 4A). Upon examination of circulating BCG-specific CD4+ T cells (reactive to M. tuberculosisCF+ rAg85A stimulation), we found that they were not strikingly increased in aerosol and i.m. vaccine groups, although the trend was higher in i.m. group (Supplemental Figure 4, B and C), and AUC values did not differ significantly between aerosol and i.m. groups (LD aerosol, P = 0.0870; HD aerosol, P = 0.2666, compared with i.m.). However, LD and HD aerosol vaccination had a significant enhancing effect on the polyfunctionality of preexisting circulating BCG-specific CD4+ T cells (Supplemental Figure 4C). Similar to BCG-specific circulating CD4+ T cells (Supplemental Figure 4B), BCG-specific circulating CD8+ T cells were not significantly increased by either aerosol or i.m. vaccination (Supplemental Figure 4D). These data indicate that, besides markedly induced mucosal T cell immunity (Figures 3 and 4), respiratory mucosal vaccination via inhaled aerosol, particularly LD aerosol, can also induce systemic polyfunctional CD4+ T cell responses, similar to i.m. route of vaccination in previously BCG-vaccinated humans. Preexisting and vaccine-induced anti-AdHu5 Ab in the circulation and airways. The high prevalence of circulating preexisting antibodies (Ab) against AdHu5 in human populations may negatively impact the potency of AdHu5-vectored vaccines following i.m. administration (20). However, little is known about its effect on the potency of AdHu5-vectored vaccine delivered via the respiratory mucosa. To address this question, we first examined the levels of AdHu5-specific total IgG in the circulation and airways (BALF) before and after vaccination (wk0 versus wk4 in circulation; wk0 versus wk8 in BALF). In keeping with our previous findings (8), there were significant levels of preexisting circulating AdHu5-specific total IgG in most of the trial participants (1 × 104 to 1 × 105), and the levels were comparable between the groups (using Kruskal-Wallis test P = 0.2048; Table 4). These titres significantly increased after HD aerosol or i.m. AdHu5Ag85A vaccination but not after LD aerosol vaccination. In comparison, preexisting levels of anti-AdHu5 total IgG in the airways were 1 to 1.5 log less than the levels in the circulation and were comparable between groups (using Kruskal-Wallis test, P = 0.2048). Of interest, LD and HD aerosol, as well as i.m. vaccination, did not alter the preexisting anti-AdHu5 total IgG levels in the airways (Table 4), but the data from HD aerosol and i.m. groups should be interpreted with caution due to the small sample size at 8 weeks. Table 4Anti-Ad5 antibody titers before and after LD aerosol, HD aerosol, and i.m. vaccination. Because the total anti-AdHu5 Ab titres may not always correlate with AdHu5-neutralizing capacity in the circulation (8), we further assessed the AdHu5-neutralizing Ab (nAb) titres before and after vaccination in the circulation and airways by using a bioassay. The preexisting AdHu5 nAb titres in the circulation were comparable between groups (using Kruskal-Wallis test, P = 0.3588) with 27%, 54%, and 66% of participants in LD, HD, and i.m. groups having > 1 × 102 AdHu5 nAb titres, respectively. Of interest, while i.m. vaccination with AdHu5Ag85A significantly increased the circulating AdHu5 nAb titers by an average of 1.5 logs, LD or HD aerosol vaccination had no such effect (Table 4). On the other hand, similar to total anti-AdHu5 IgG levels, preexisting AdHu5 nAb titers in the airways were ~1 log less than those in the circulation (Table 4). Of importance, 63%, 36%, and 33% of participants in LD, HD., and i.m. groups, respectively, had no detectable baseline AdHu5 nAb titers in their airways, which remained unaltered following vaccination (Table 4). We further found a significant positive correlation between AdHu5 nAb and total AdHu5 IgG titres both in the circulation and airways (Supplemental Figure 5, A and B). Given that many of the trial participants had moderate to significant levels of AdHu5 nAb titers in the circulation and ~50% of them also had a small but detectable level of preexisting AdHu5 nAb titres in the airways, we next examined whether such nAbs present in the airways and blood may have negatively impacted the immunopotency of LD aerosol and i.m. vaccination, respectively. To this end, the percentage of airways or blood with total-cytokine+ Ag85A-specific CD4+ T cells at the peak response time (2 weeks post-vaccination) for individual participants was plotted against corresponding preexisting AdHu5 nAb titres, and Spearman rank correlation test was performed. There was no significant correlation between preexisting airways AdHu5 nAb titers and the magnitude of vaccine-induced CD4+ (Supplemental Figure 5C) and CD8+ (Supplemental Figure 5D) T cell responses in the airways following LD aerosol vaccination. Of note, one participant who hardly responded to aerosol vaccine did have the highest neutralization titers in the cohort (Supplemental Figure 5, C and D). On the other hand, consistent with our previous observation (8), there was no significant correlation between preexisting circulating AdHu5 nAb titers and the magnitude of antigen-specific CD4+ (Supplemental Figure 5E) and CD8+ (Supplemental Figure 5F) T cell responses in the blood following i.m. vaccination. The above data suggest that, while there is high prevalence of preexisting circulating anti-AdHu5 nAb in humans enrolled in our study, most trial participants have either undetectable or very low levels of preexisting anti-AdHu5 nAb titers in the airways. I.m. AdHu5Ag85A vaccination increases AdHu5 nAb titers in the circulation, whereas aerosol vaccination does not do so either in the airways or in the circulation. Although the presence of AdHu5 nAb in the airways does not seem to have a significant impact on aerosol vaccine immunogenicity, the data should be interpreted with caution due to the small sample size and very few BALF samples with significant AdHu5 nAb titers.
|
|
Scooped by
Gilbert C FAURE
October 3, 2022 3:47 AM
|
Clinical Trial of BioBlock COVID-19 Nasal Spray Containing Anti-SARS-CoV-2 Antibodies Derived From Bovine Colostrum - Full Text View.
|
|
Scooped by
Gilbert C FAURE
September 5, 2022 2:43 PM
|
Cansino Biologics' inhaled vaccine appeared more effective in clinical trials than China's other jabs.
|
|
Scooped by
Gilbert C FAURE
August 21, 2022 2:44 AM
|
A small spray in to the nose could protect people from COVID-19 and hamstring the pandemic, but the science still faces major challenges.
|
|
Scooped by
Gilbert C FAURE
August 18, 2022 5:11 AM
|
Analysis: a bivalent vaccine has been approved and research is being carried out into possible pan-coronavirus vaccines...
|
|
Scooped by
Gilbert C FAURE
August 13, 2022 11:08 AM
|
The mRNA vaccine platform has offered the greatest potential in fighting the COVID-19 pandemic owing to rapid development, effectiveness, and scalability to meet the global demand. There are many other mRNA vaccines currently being developed against different emerging viral diseases. As with the current COVID-19 vaccines, these mRNA-based vaccine candidates are being developed for parenteral administration via injections. However, most of the emerging viruses colonize the mucosal surfaces prior to systemic infection making it very crucial to target mucosal immunity. Although parenterally administered vaccines would induce a robust systemic immunity, they often provoke a weak mucosal immunity which may not be effective in preventing mucosal infection. In contrast, mucosal administration potentially offers the dual benefit of inducing potent mucosal and systemic immunity which would be more effective in offering protection against mucosal viral infection. There are however many challenges posed by the mucosal environment which impede successful mucosal vaccination. The development of an effective delivery system remains a major challenge to the successful exploitation of mucosal mRNA vaccination. Nonetheless, a number of delivery vehicles have been experimentally harnessed with different degrees of success in the mucosal delivery of mRNA vaccines. In this review, we provide a comprehensive overview of mRNA vaccines and summarise their application in the fight against emerging viral diseases with particular emphasis on COVID-19 mRNA platforms. Furthermore, we discuss the prospects and challenges of mucosal administration of mRNA-based vaccines, and we explore the existing experimental studies on mucosal mRNA vaccine delivery.
|
|
Scooped by
Gilbert C FAURE
July 28, 2022 4:47 AM
|
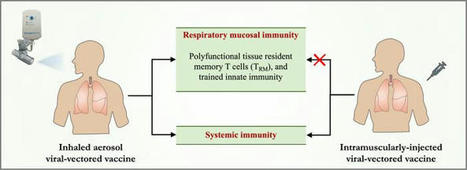
researchers assess the respiratory mucosal immunity elicited by COVID-19 vaccination.
|
|
Scooped by
Gilbert C FAURE
July 21, 2022 3:43 AM
|
Our inhaled COVID-19 vaccine would go directly to where the body needs it: the surface of the airways. This means less waste and more benefit, lower costs and reduced side-effects.
Les chercheurs du Laboratoire commun Institut Pasteur-TheraVectys ont montré l’efficacité de leur candidat vaccin lentiviral «Lenti-COVID», administré en dose de rappel par voie nasale, six mois après la primo-vaccination par un vaccin à ARN messager, dans un modèle pré-clinique. Ce rappel intranasal induit une immunité protectrice au niveau des muqueuses respiratoires. Ces résultats ouvrent la voie à une stratégie vaccinale innovante propice à la réduction de la chaîne de transmission virale.
Via HAS-veille
|
|
Scooped by
Gilbert C FAURE
April 26, 2022 1:52 PM
|
Although SARS-CoV-2 infects the upper respiratory tract, we know little about the amount, type, and kinetics of antibodies (Ab) generated in the oral cavity in response to COVID-19 vaccination. We collected serum and saliva samples from participants receiving two doses of mRNA COVID-19 vaccines and measured the level of anti-SARS-CoV-2 Ab. We detected anti-Spike and anti-Receptor Binding Domain (RBD) IgG and IgA, as well as anti-Spike/RBD associated secretory component in the saliva of most participants after dose 1. Administration of a second dose of mRNA boosted the IgG but not the IgA response, with only 30% of participants remaining positive for IgA at this timepoint. At 6 months post-dose 2, these participants exhibited diminished anti-Spike/RBD IgG levels, although secretory component-associated anti-Spike Ab were more stable. Examining two prospective cohorts we found that participants who experienced breakthrough infections with SARS-CoV-2 variants had lower levels of vaccine-induced serum anti-Spike/RBD IgA at 2–4 weeks post-dose 2 compared to participants who did not experience an infection, whereas IgG levels were comparable between groups. These data suggest that COVID-19 vaccines that elicit a durable IgA response may have utility in preventing infection. Our study finds that a local secretory component-associated IgA response is induced by COVID-19 mRNA vaccination that persists in some, but not all participants. The serum and saliva IgA response modestly correlate at 2–4 weeks post-dose 2. Of note, levels of anti-Spike serum IgA (but not IgG) at this timepoint are lower in participants who subsequently become infected with SARS-CoV-2. As new surges of SARS-CoV-2 variants arise, developing COVID-19 booster shots that provoke high levels of IgA has the potential to reduce person-to-person transmission.
|
|
Scooped by
Gilbert C FAURE
March 4, 2022 1:00 PM
|
Alors que le monde attend des thérapies efficaces contre la COVID-19, des chercheurs de l'Académie chinoise des sciences affirment avoir mis au point un...
|
|
Scooped by
Gilbert C FAURE
February 12, 2022 1:37 PM
|
Abstract Exacerbated pro-inflammatory immune response contributes to COVID-19 pathology. However, despite the mounting evidence about SARS-CoV-2 infecting the human gut, little is known about the a...
|
|
Scooped by
Gilbert C FAURE
January 19, 2022 5:04 AM
|
The mucosal immune system is the largest component of the entire immune system, having evolved to provide protection at the main sites of infectious threat: the mucosae. As SARS-CoV-2 initially infects the upper respiratory tract, its first interactions with the immune system must occur...
|
|
|
Scooped by
Gilbert C FAURE
October 12, 2022 6:10 AM
|
Systemic and mucosal humoral immune responses are crucial to fight respiratory viral infections in the current pandemic of COVID-19 caused by the SARS-CoV-2 virus. During SARS-CoV-2 infection, the dynamics of systemic and mucosal antibody infections are affected by patient characteristics, such as age, sex, disease severity, or prior immunity to other human coronaviruses. Patients suffering from severe disease develop higher levels of anti-SARS-CoV-2 antibodies in serum and mucosal tissues than those with mild disease, and these antibodies are detectable for up to a year after symptom onset. In hospitalized patients, the aberrant glycosylation of anti-SARS-CoV-2 antibodies enhances inflammation-associated antibody Fc-dependent effector functions, thereby contributing to COVID-19 pathophysiology. Current vaccines elicit robust humoral immune responses, principally in the blood. However, they are less effective against new viral variants, such as Delta and Omicron. This review provides an overview of current knowledge about the humoral immune response to SARS-CoV-2, with a particular focus on the protective and pathological role of humoral immunity in COVID-19 severity. We also discuss the humoral immune response elicited by COVID-19 vaccination and protection against emerging viral variants.
|
|
Scooped by
Gilbert C FAURE
September 15, 2022 2:03 PM
|
Protection against Omicron by Mucosal IgA Antibodies In this study, a mucosal IgA response to three doses of mRNA Covid-19 vaccine was associated with a reduced risk of infection. Induction o
|
|
Scooped by
Gilbert C FAURE
September 5, 2022 2:42 PM
|
China’s National Medical Products Administration approved CanSino’s Ad5-nCoV for emergency use as a booster vaccine.
|
|
Rescooped by
Gilbert C FAURE
from Virus World
August 18, 2022 2:04 PM
|
One ‘superspreader’ with Omicron shed three times as much viral RNA as those with Alpha or Delta. People infected with the highly transmissible Alpha, Delta and Omicron variants of SARS-CoV-2 spew out higher amounts of virus than do those infected with other variants, according to a study1. Furthermore, individuals who contract COVID-19 after vaccination, and even after a booster dose, still shed virus into the air. The work was posted on the medRxiv preprint server on 29 July. It has not yet been peer reviewed. “This research showed that all three of those variants that have won the infection race … come out of the body more efficiently when people talk or shout than the earliest strains of the coronavirus,” says John Volckens, a public-health engineer at Colorado State University in Fort Collins. Study co-author Kristen Coleman, who researches emerging infectious diseases at the University of Maryland in College Park, says this means that people should be “pushing governments to invest in improving indoor air quality by improving ventilation and filtration systems”. Breathe out For the study, Coleman and her colleagues recruited 93 people between mid-2020 and early 2022 who were infected with SARS-CoV-2. Participants’ infections were caused by strains including the Alpha variant, which emerged in late 2020, and the later Delta and Omicron variants. All participants with the latter two strains had been fully vaccinated before catching the virus. The infected people faced into a cone-shaped apparatus and sang and shouted — with inevitable coughs and sneezes in between — for 30 minutes, while an attached machine collected the particles they exhaled. The device, called a Gesundheit-II, separated out the fine ‘aerosol’ droplets measuring 5 micrometres or less in diameter, which can linger in the air and leak through cloth and surgical masks. The team found that participants infected with the Alpha, Delta and Omicron variants emitted significantly more viral RNA when exhaling than did people infected with other variants. These include ancestral variants, such as the one first detected in Wuhan, China, and those not associated with increased transmissibility — such as Gamma, which arose in late 2020. For participants with Delta and Omicron, their fine aerosol contained on average five times the amount of virus that was detected in their larger, coarse aerosol. The team also seeded cells in the laboratory with aerosol samples and found that four samples, each from a participant with either Delta or Omicron, infected the cells. Shed virus is not always infectious, says study co-author Jianyu Lai, an epidemiologist at the University of Maryland, and the samples’ ability to infect laboratory cells means that viral RNA in exhaled aerosols can spread the disease. Malin Alsved, an aerosol technology scientist at Lund University in Sweden, says: “I’m bit concerned that they mix all the respiratory [aerosols] — they have breathing, talking, speaking, screaming, coughing, even sneezing in the sample.” Coleman responds that the team combined respiratory samples to mimic a real-life scenario such as being in a restaurant. Going viral The study also highlights variation between individuals in the amounts of exhaled virus, which ranged from non-detectable levels to those associated with ‘superspreaders’. One Omicron-infected participant, for example, shed 1,000 times as much viral RNA through fine aerosol as the maximum level observed in those with Alpha or Delta. The researchers say that the root of these discrepancies remains a mystery but could be related to biological factors such as a person’s age. Behaviour might play a part, too: the study’s superspreader coughed more frequently than others. If new variants are more prone to superspreading, that might drive them to dominate COVID-19 cases. The team notes that people infected with SARS-CoV-2 exhale much lower amounts of viral RNA than do people infected with influenza, a comparable airborne disease. This suggests that SARS-CoV-2 could spin off variants that transmit even more virus. “That is something to be concerned about,” says Alsved. Published in Nature (August 17, 2022): https://doi.org/10.1038/d41586-022-02202-z
Via Juan Lama
|
|
Scooped by
Gilbert C FAURE
August 18, 2022 5:07 AM
|
Longitudinal analysis of T cell, B cell, and antibody response to four different COVID-19 vaccines in humans, representing three different vaccine technologies, identifies different quantities and quality of CD4+ T cell, CD8+ T cell, and antibody response elicited by mRNA-1273, BNT162b2,...
|
|
Scooped by
Gilbert C FAURE
July 28, 2022 4:49 AM
|
SARS-CoV-2 typically enters the body via the nose or mouth. Because of this, many think a nasal spray vaccine would do a better job of preventing COVID-19 infection and cutting transmission than an injection.
|
|
Scooped by
Gilbert C FAURE
July 27, 2022 3:27 AM
|
The White House on Tuesday held a summit with vaccine makers and scientists as it pushed for "next generation" COVID-19 vaccines that offer broader and more durable protection against the virus.
|
|
Scooped by
Gilbert C FAURE
May 25, 2022 2:19 AM
|
Un essai clinique réalisé en Chine a montré qu'un vaccin de rappel contre la COVID-19 à inhaler est sûr et efficace chez les adultes. Les scientifiques...
|
|
Scooped by
Gilbert C FAURE
May 12, 2022 11:23 AM
|
Scientists are studying whether long COVID could be linked to viral fragments found in the body months after initial infection
|
|
Scooped by
Gilbert C FAURE
March 29, 2022 3:37 AM
|
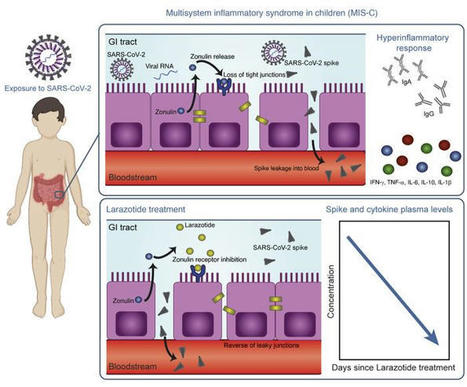
This study included biospecimens from 100 children: 19 children were clinically diagnosed with MIS-C as defined by CDC criteria (Supplemental Table 1; supplemental material available online with this article; https://doi.org/10.1172/JCI149633DS1); 26 children had COVID-19 confirmed by RT-PCR; and 55 children served as non–COVID-19 controls (32 pre-pandemic). The average age of the children with MIS-C (8 years old) was younger than that of the children who presented with COVID-19 (14 years old), which is consistent with the national averages (2, 15). The patients with MIS-C presented with a median of 3 days of acute symptoms associated with MIS-C (range, 1–28 days), after a previous COVID-19 exposure or SARS-CoV-2 infection 26 days prior to the presentation with MIS-C (range, 13–62 days). Notably, GI symptoms were predominant in the MIS-C cohort, affecting 89% of these patients, compared with 27% of children with acute COVID-19 (Fisher’s exact test, P < 0.0001; Table 1). Figure 1 outlines the specimens collected for the analysis and the timing of specimen collection from the children with MIS-C or acute COVID-19. Figure 1Study overview. Timing of sample collection and sample analysis for children with MIS-C or acute COVID-19. Table 1Age and sex for all pediatric patients and controls, and clinical features of illness for the children with acute COVID-19 or MIS-C SARS-CoV-2 in the GI tract of children with MIS-C coincides with a loss of intestinal epithelial barrier function. MIS-C develops several weeks after a SARS-CoV-2 infection or exposure (Table 1), and the viral load in respiratory secretions is known to decrease over the course of 7–10 days after infection (11, 16, 17). As most children with MIS-C have negative nasopharyngeal viral swabs (11), MIS-C is unlikely to be related to this initial infection of the respiratory tract. To assess the presence of SARS-CoV-2 in the GI tract, we measured SARS-CoV-2 RNA from MIS-C stool samples collected several weeks after the initial SARS-CoV-2 infection or exposure. Indeed, a majority of the patients showed detectable viral loads in the stool ranging from 1.5 × 102 to 2.5 × 107 RNA copies/mL, suggesting an ongoing nidus of infection in MIS-C (Supplemental Table 1). An intact, functional intestinal mucosal barrier should prevent the passage of large antigens from the gut lumen into the bloodstream, including viral antigens derived from SARS-CoV-2 present in the GI tract (12). Zonulin belongs to a family of structurally and functionally related proteins that reversibly regulate intestinal permeability by modulating intercellular tight junctions (18–20). Increased circulating zonulin levels resulting in increased intestinal permeability have been reported in several diseases (21) including autoimmune and hyperinflammatory diseases such as celiac disease (22), inflammatory bowel disease (23), and Kawasaki disease (24). Zonulin release from epithelial cells can result in permissibility of paracellular trafficking of large inflammatory antigens from the gut lumen into the bloodstream. In this study, mass spectrometry showed that, compared with controls, children with MIS-C had significantly increased release of zonulin into the circulation (P = 0.003; Figure 2A), which can result in a breakdown of mucosal barrier function. Correspondingly, children with MIS-C also had increased LPS-binding protein (LBP) levels compared with controls (P = 0.007; Figure 2B), signaling increased microbial translocation. Levels of soluble CD14, another marker of microbial translocation, were also increased in children with MIS-C (P = 0.1; Figure 2C), indicating a loss of GI mucosal barrier integrity. None of these markers of GI barrier integrity — zonulin, LBP, or CD14 — was significantly increased in the children with acute COVID-19 infection. Identification of SARS-CoV-2 within the stool, coupled with the loss of competency of tight junctions seen in MIS-C, but not acute COVID-19, suggests that GI sources of SARS-CoV-2 viral components could breach the mucosal barrier and enter the circulation. Figure 2Plasma (A) zonulin, (B) LPS-binding protein, and (C) soluble CD14 levels were quantified by multiplexed MS–based proteomics (54, 55) for children with MIS-C (n = 13) or COVID-19 (n = 21) and for non–COVID-19 control participants (n = 23). Results were compared by ANOVA. (D) SARS-CoV-2 spike, (E) S1, and (F) nucleocapsid protein levels were quantified in plasma from children with MIS-C (n = 16), children with acute COVID-19 (n = 22), and pre-pandemic healthy controls (n = 32). Results were compared by 1-way ANOVA with multiple comparisons. * P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001. Median values and 95% CI are presented. Children with MIS-C have SARS-CoV-2 antigenemia. Although viremia and antigenemia have been shown to correlate with severe acute COVID-19 in adults (17, 25), viremia has not been detected in MIS-C (11), and antigenemia has not previously been assessed in children. Using single-molecule array (Simoa) assays (25), we detected SARS-CoV-2 spike, S1, and nucleocapsid antigens in the plasma of children with MIS-C despite being weeks past their initial SARS-CoV-2 infection or exposure. The SARS-CoV-2 spike protein was significantly elevated in patients with MIS-C compared with healthy controls (P < 0.0001) and compared with children with acute COVID-19 (P < 0.001; Figure 2D). We also detected the SARS-CoV-2 S1 protein at significantly elevated levels in patients with MIS-C compared with healthy controls (P = 0.004) and with children with acute COVID-19 (P = 0.02; Figure 2E). SARS-CoV-2 nucleocapsid protein levels were increased in patients with MIS-C, although these levels did not reach significance (Figure 2F). We detected no significant increase in SARS-CoV-2 antigenemia in children with acute COVID-19 as compared with healthy controls. SARS-CoV-2 antigens showed no correlation with age (Supplemental Figure 1). Circulating SARS-CoV-2 antigen indicates that viral components have leaked from infected tissues. We attribute circulating antigen in patients with MIS-C to leakage from the GI system, as corroborated by the increased zonulin levels and microbial translocation markers we detected in the patients with MIS-C. The SARS-CoV-2 spike protein, specifically the S1 component (9, 10), has been hypothesized to have superantigen-like properties that are similar to those seen in the bacterial superantigen–mediated toxic shock syndrome. Superantigens bind to specific β-chains of T cell receptors (TCRs) at the variable domain in a complementary-determining region 3–independent (CDR3-independent) manner (26), thereby bypassing TCR specificity and resulting in skewing and overrepresentation of specific TCRs. Recent reports have identified TCR β variable (TRBV) gene skewing in MIS-C, with a profound expansion of TRBV11-2 (10, 27). Our data reveal a strong correlation between S1 antigenemia and the previously reported expression of TRBV11-2 in MIS-C (ref. 10; Pearson’s correlation, r = 0.89, P = 0.0005; Supplemental Figure 2). We found no correlation between the spike or nucleocapsid antigens and TRBV11-2 expression (Supplemental Figure 2). Consistent with hyperinflammatory responses, children with MIS-C experienced a cytokine storm with significantly elevated levels of IL-1β, IL-6, IL-10, and TNF-α (Supplemental Figure 3, A–D). Notably, the antiviral cytokine IFN-γ was also significantly increased in patients with MIS-C compared with both healthy controls and children with acute COVID-19 (Supplemental Figure 3E). This increase in IFN-γ is typical of a viral exposure, however, it can be paradoxically suppressed in adults with severe acute COVID-19 (28). We also assessed IL-12p70, IL-8, IL-5, and IL-22 levels but found that they were not altered in the children with MIS-C or acute COVID-19 (Supplemental Figure 3, F–I). MIS-C immunoprofiles reflect ongoing mucosal exposure to SARS-CoV-2. The immunoglobulin IgM, IgG, and IgA subsets targeting SARS-CoV-2 antigens in patients with MIS-C were most highly elevated against spike and S1 proteins (Figure 3, A–C, and Supplemental Figure 4), corresponding to the antigens most highly detected in the bloodstream of these children. As expected, anti–spike IgM was highest in children with acute COVID-19, reflecting early adaptive immune responses (Figure 3A). However, anti–spike IgM levels remained higher than would be expected, given that MIS-C presents weeks after the original infection with or exposure to SARS-CoV-2, but was on a downward trend over time (Figure 3D). As expected, anti–spike IgG, anti–S1 IgG, and anti–RBD IgG were highest in the children with delayed-onset MIS-C (Figure 3B and Supplemental Figure 4) and remained plateaued over time (Figure 3E). IgA is the immunoglobulin most reflective of mucosal immunity and typically wanes following viral clearance (29). Here, the levels of anti–spike IgA, anti–S1 IgA, and anti–RBD IgA were all significantly increased in the patients with MIS-C (Figure 3C and Supplemental Figure 4), and anti–spike IgA remained unexpectedly elevated for months after the initial SARS-CoV-2 infection (Figure 3F). The persistence of elevated anti–SARS-CoV-2 IgA and IgM in patients with MIS-C supports the hypothesis of ongoing viral antigenic exposure and inflammation in the GI mucosal surfaces of children with MIS-C. Figure 3Peak values of (A) anti–spike IgM, (B) anti–spike IgG, and (C) anti–spike IgA were quantified in plasma from children with MIS-C (n = 16), children with acute COVID-19 (n = 22), and pre-pandemic healthy controls (n = 32). Results were compared by 1-way ANOVA with multiple comparisons. Time course of (D) anti–spike IgM, (E) anti–spike IgG, and (F) anti–spike IgA were plotted over time following symptom onset for MIS-C. (G) The IC50 for antibody neutralization for children with MIS-C and children with acute COVID-19 were compared by Mann-Whitney t test. Mean values and the SD are presented. *P < 0.05, **P < 0.01, and ****P < 0.0001. We compared the capacity of plasma neutralization against SARS-CoV-2 between children with MIS-C and those with acute COVID-19. Interestingly, although the children with MIS-C had significantly elevated IgG antibody titers against SARS-CoV-2 relative to those with acute COVID-19, the neutralization titers were comparable between the children from both groups (Figure 3G). This suggests that in children with MIS-C, increasing quantities of IgG antibodies against the SARS-CoV-2 spike protein did not result in a gain in neutralizing capacity over time. Ineffective neutralization and poor antigen clearance, combined with ongoing viral antigen leakage from GI sources, could partially explain the high levels of antigen detected in the children with MIS-C. Temporal kinetics reveal that SARS-CoV-2 antigenemia is inadequately contained by humoral responses in MIS-C. Both SARS-CoV-2 antigen and immunoglobulins were detectable in patients with MIS-C at levels significantly higher than those detected in healthy controls. Antigenemia in adults occurs early in the COVID-19 disease course and is associated with pulmonary symptoms (25), whereas in MIS-C, antigenemia is found in the setting of prominent GI symptoms weeks to months after resolution of a SARS-CoV-2 upper respiratory tract infection or asymptomatic infection. To understand the relationship between viral antigenemia and the humoral response, we studied longitudinal samples from patients with MIS-C. First, we assessed antigens over time following MIS-C symptom onset. Previous reports show that in adults with acute COVID-19, SARS-CoV-2 antigens are rapidly cleared as the patient reaches seroconversion (25, 30). In contrast, our studies showed that spike antigens rose over the first few days of MIS-C symptoms and persisted for more than 10 days, occasionally through 6 months (Supplemental Figure 5), despite seroconversion to anti–spike IgG and anti–spike IgA antibodies. The elevated presence of spike protein in seroconverted patients was not observed in any adult COVID-19 cases (25). We also found that SARS-CoV-2 antigen levels did not significantly decrease in our cohort following the initiation of steroid and/or intravenous immunoglobulin (IVIG) replacement therapy (Figure 4A), which are the only currently recommended treatments for MIS-C (31). This suggests that current therapies are targeted toward the downstream consequences of MIS-C, namely the inflammatory responses, but fail to address the ongoing antigenemia instigating ongoing inflammation. Figure 4B provides a detailed overview of spike antigenemia and the humoral inflammatory responses in a representative hospitalized child with MIS-C, relative to SARS-CoV-2 exposure, symptom onset, and treatment course. Figure 4(A) SARS-CoV-2 spike, S1, and nucleocapsid levels in plasma from children with MIS-C were quantified before treatment with steroids and/or immunoglobulin replacement therapy, through 14 days following treatment (n = 11). Shaded regions signify the limit of detection for each specific antigen test. (B) Spike and anti–spike IgM, anti–spike IgG, and anti–spike IgA levels were measured over the course of illness of a child with MIS-C. Of note, the spike protein remained above the limit of detection for the spike antigen test at the 213-day follow-up point. Zonulin antagonism reduces spike antigenemia and cytokine storm, with subsequent improvement in clinical outcomes in MIS-C. Although steroids and IVIG do not block leakage of SARS-CoV-2 antigen across the mucosal barrier, therapies targeting GI mucosal permeability could potentially reduce or prevent antigenemia. Larazotide, a zonulin antagonist, is an investigational therapy that has been well characterized in preclinical trials (32, 33), with an excellent safety profile (34), and is currently in phase III trials for the treatment of refractory celiac disease (35). Given this theoretical benefit, we obtained US FDA approval for compassionate use of larazotide, 10 μg/kg every 6 hours, to treat a critically ill 17-month-old boy with MIS-C after he failed to improve with antiinflammatory therapies. The toddler, who had a complex past medical history including partial duplication of chromosome 14, biliary atresia status post Kasai procedure, and gastrotomy tube placement, with frequent episodes of ascending cholangitis, required hospitalization for severe COVID-19, complicated by respiratory failure and cardiac resuscitation. One month after he was diagnosed with COVID-19, he developed abdominal compartment syndrome with a C-reactive protein (CRP) level of 286 mg/L, a ferritin level of 51,223 μg/L, and a N-terminal pro-b–type natriuretic peptide (NT-proBNP) level of 16,462 pg/mL without evidence of cardiac injury on echocardiogram. He was treated with IVIG, steroids, and anakinra with transient improvement of inflammatory markers but rapid recrudescence of symptoms. We detected 1020 copies of SARS-CoV-2 RNA in the patient’s stool, as quantified by RT-PCR, and a plasma spike antigen level of 566 pg/mL more than 2 weeks after initiation of IVIG and steroid treatment for MIS-C. After the initiation of larazotide, his CRP level, which had quickly rebounded to 173 mg/L following withdrawal of anakinra, dropped by 85% from peak values, and spike antigen levels dropped by 90% to 59 pg/mL (Figure 5A). The SARS-CoV-2 nucleocapsid protein levels also dropped by 98% from 77 pg/mL to 1.45 pg/mL (limit of detection). His fever curve, which also rebounded after discontinuation of anakinra, improved, as did his ferritin and D-dimer levels (Figure 5A). The patient also experienced an improvement in cytokine and inflammatory mediator levels, including IL-1β, IFN-γ, IL-2R, and IL-17, representing an improvement in inflammasome activation, virus-induced IFN release, and immune cell activation (Figure 5B). These cytokines and inflammatory mediators initially spiked during the development of MIS-C, then improved following IVIG but plateaued or rebounded despite steroid treatment. We observed an improvement in these inflammatory mediators following the precipitous drop in SARS-CoV-2 antigens, which occurred as a result of or coincident with the initiation of larazotide therapy. Importantly, the patient achieved his longest stretches without fever since his hospital admission, his GI symptoms improved and he was able to resume full feedings, and his ventilatory status improved. Figure 5Timeline for the child treated with larazotide. The hospital course is delineated by hospitalization for acute COVID-19 (day 0) followed by development of MIS-C (day 39), with the treatment courses identified along the time course. (A) CRP and SARS-CoV-2 spike antigen levels, the median daily temperature (temp) curve, and D-dimer and ferritin levels throughout the hospital course are shown. Light blue shading represents a normal body temperature. The light gray shading highlights the days of larazotide treatment. (B) Inflammatory cytokine IL-17F, IL-2R, IFN-γ, and IL-1β levels following the development of MIS-C, in relation to the treatment courses.
|
|
Scooped by
Gilbert C FAURE
February 19, 2022 10:48 AM
|
Here, we developed an in situ RNA detection assay for RNA generated by the SARS-CoV-2 virus. We found viral RNA in lung, lymph node, and placenta samples from pathology specimens from COVID patient...
|
|
Scooped by
Gilbert C FAURE
January 28, 2022 6:20 AM
|
SARS-CoV-2 infection is benign in most individuals but, in ˜10% of cases, it triggers hypoxemic COVID-19 pneumonia, which becomes critical in ˜3% of cases. The ensuing risk of death (˜1%) doubles every five years from childhood onward and is ˜1.5 times greater in men than in women. What are the molecular and cellular determinants of critical COVID-19 pneumonia? Inborn errors of type I IFNs, including autosomal TLR3 and X-linked TLR7 deficiencies, are found in ˜1-5% of patients with critical pneumonia under 60 years old, and a lower proportion in older patients. Pre-existing autoantibodies neutralizing IFN-α, –β, and/or –ω, which are more common in men than in women, are found in ˜15-20% of patients with critical pneumonia over 70 years old, and a lower proportion in younger patients. Thus, at least 15% of cases of critical COVID-19 pneumonia can apparently be explained. The TLR3- and TLR7-dependent production of type I IFNs by respiratory epithelial cells and plasmacytoid dendritic cells, respectively, is essential for host defense against SARS-CoV-2. In ways that can depend on age and sex, insufficient type I IFN immunity in the respiratory tract during the first few days of infection may account for the spread of the virus, leading to pulmonary and systemic inflammation.
|