Your new post is loading...

|
Scooped by
Juan Lama
June 24, 2025 10:48 AM
|
RetroVirox has launched a Summer Promotion with a 30% discount for antiviral and neutralization services against 4 viruses, including influenza, dengue, human metapneumovirus (HMPV) and respiratory syncytial virus (RSV). Discount applies to services initiated between July 1 and August 31 2025
Contact us at info@retrovirox.com for inquiries and additional info
|
|
Scooped by
Juan Lama
May 28, 6:26 PM
|
A 6-month regimen of an experimental drug for the hepatitis B virus (HBV) added to standard antivirals has “functionally cured” 19% of people in two efficacy trials, meaning they can naturally control that virus without any further treatments. The results, published today in The New England Journal of Medicine (NEJM) and presented at Europe’s largest meeting on liver health, come from people whose chronic HBV infections were already relatively well controlled with the existing drugs, so its effectiveness in other populations that are more challenging to treat remains unknown. The findings are “remarkable” and “a major step” forward for the field, hepatologist Anna Lok of the University of Michigan Medical School wrote in an editorial accompanying the NEJM editorial—although she cautioned it was far from a solution to a major global problem. GSK in January had announced that its drug, called bepirovirsen (bepi), had positive results in two phase 3 efficacy trials that involved more than 1800 participants in 29 countries, but the company did not report any details. Many researchers anticipated that about 10% of trial participants would achieve natural suppression of HBV—what the field calls a functional cure—as that’s what was found in the earlier phase 2 bepi trials. The even more impressive result is “exciting news,” says Nick Walsh, an epidemiologist at Monash University who specializes in hepatitis diseases and was unconnected to the study. “This will certainly bring much needed attention to HBV and should accelerate further efforts to find a cure, which indeed needs to be urgently rolled out,” he says. But Walsh and other HBV researchers stress that bepi’s unprecedented powers may well have a limited impact for most of the 240 million people worldwide living with chronic HBV infections, which kill 1.1 million each year. The World Health Organization estimates only 27% of infected people have been diagnosed, and of those, fewer than 5% receive treatment. Chronic HBV infections can destroy the liver and ultimately kill if left unchecked. They currently require lifelong treatment, and less than 1% of patients who receive existing drugs can control the virus after stopping treatments. The most commonly used HBV drugs disrupt the ability of the virus to make copies of its genes by introducing into infected cells defective analogs of the nucleosides or nucleotides—nukes—that make up its DNA. Bepi, in contrast, is an antisense oligonucleotide that derails viral replication by binding to HBV’s messenger RNA, preventing it from making needed proteins and triggering its destruction. The drug separately stimulates immune responses against the virus. The new phase 3 studies focused on the subset of the treated population for whom the standard drugs were working. Participants had relatively low levels of the viral surface protein, or antigen, in their blood and did not have HIV infections or liver scarring known as cirrhosis. Two-thirds of participants added bepi shots for 24 weeks to their daily nuke pills, while a control group added placebo shots. Everyone then continued with nukes for another 24 weeks. Six months after stopping all treatment, 233 of 1220 people who had received bepi had functional cures—both undetectable HBV DNA and surface antigen—versus zero of 614 participants in the placebo arm. The functional cure rate went up to 26% in participants who entered the study with the lowest levels of the viral surface antigen. Side effects were common, but rarely severe. When HBV infects adults, typically through sex or sharing needles during drug use, the immune system clears the virus about 90% of the time. In infants who become infected, mainly by mother-to-child transmission, their less mature immune systems falter more often—90% develop chronic infections. An infection becomes chronic when HBV integrates its DNA into human chromosomes and also forms an intractable miniature chromosome inside cells called cccDNA. Like the nukes, bepi doesn’t eliminate the embedded cccDNA—a “sterilizing” cure—but it helps suppress HBV levels to low enough levels for a long enough period to reinvigorate immune responses against the virus. Many researchers see the functional cure bepi provides as a more realistic goal than a sterilizing cure. The new results are “a long-awaited milestone in the journey toward curing HBV infection,” says Fabien Zoulim, a hepatologist at Claude Bernard University Lyon 1. Whether a bepi-induced functional cure is lifelong remains a key issue. Zoulim notes that the durability of surface antigen loss “requires further assessment through extended follow-up.” Data from the much smaller phase 2 studies of the drug have shown viral suppression for up to 3 years in more than 90% of the functionally cured patients, according to Melanie Paff, a GSK scientist who spoke at a press briefing last week. GSK has already submitted the new phase 3 data to drug regulatory agencies in Europe, the United States, Canada, Japan, and China. The company expects at least some approvals to occur later this year. It has yet to announce how much the drug will sell for in wealthy countries and resource-limited ones. “We are committed to pricing which balances the value of innovation and patient access, and we’ll continue to work constructively with payers around the world to achieve this,” a GSK spokesperson told Science. Despite the promise of bepi, some hepatitis B researchers remain frustrated that pharmaceutical companies have not made more of an effort to design even better, truly curative drugs. “There have not been enough collaborations within industry—each company tries to work on its own,” Lok says, “and we expect that a cure, for many patients, will require a multiprong approach.” Study published in NEJM (May 28, 2026): https://www.nejm.org/doi/full/10.1056/NEJMoa2515131
|
|
Scooped by
Juan Lama
May 26, 11:51 AM
|
A Spanish national who was evacuated from the cruise ship MV Hondius and is isolating at a hospital in Madrid has tested positive of hantavirus, Spain’s Ministry of Health said Monday. The patient is one of the 14 Spaniards who were aboard the MV Hondius. They have been in quarantine at the Gómez Ulla Central Defense Hospital in Madrid since May 10. Authorities stated that the patient is a close contact identified through the epidemiological monitoring activated after the initial detection of the outbreak on the cruise ship. After the case was confirmed, the patient was transferred to the hospital’s High-Level Isolation Unit (UATAN), where they will remain under specialized medical supervision. The patient is the second Spaniard aboard the Hondius to test positive. Following the confirmation, the health ministry sought to reassure the public, stating that the case was detected within the isolation and control system already in place. Therefore, it does not change the level of risk for the general population nor alter the epidemiological response measures currently underway. Health authorities from several countries have been racing to trace and contain the hantavirus outbreak after three passengers died following MV Hondius’ departure from Argentina in April. Dozens of passengers disembarked at the remote South Atlantic island of Saint Helena in late April while the remaining passengers left the boat at Spain’s Canary Islands in May before being flown back to their respective home countries. Additional crew members later disembarked from the ship in the Netherlands. Incubation period Infectious disease experts told CNN last week that passengers on board the ship since early May are within the window when they will be most likely to develop symptoms. “No one would be surprised if there are others that test positive this upcoming week,” said Dr. Isaac Bogoch, an infectious disease specialist and professor at the University of Toronto said at the time. The average incubation period for the virus (the time between infection and development of symptoms) is roughly three weeks, according to his research. It can take as long as six weeks for symptoms to appear, which is why most countries are monitoring passengers for a minimum of 42 days counted from the day they got off the ship. The virus is typically associated with rodents, but it may have passed from human to human aboard the vessel, according to the World Health Organization. It’s rare disease that can feel like the flu, causing fatigue, fever, chills and aches. Over time, the virus can damage the heart, lungs or kidneys and patients can suffer severe shortness of breath, organ failure, and even die.
|
|
Scooped by
Juan Lama
May 15, 12:57 PM
|
Africa’s leading public health authority said on Friday that there was an outbreak of the Ebola virus in a province of the Democratic Republic of Congo, with dozens of deaths and hundreds of infections suspected. The Africa Centers for Disease Control and Prevention, the public health agency of the African Union, said 65 deaths from Ebola had been reported in the northeastern province of Ituri, though only four had been definitively linked to the virus through laboratory testing. The agency said that 246 suspected infections had been reported in Ituri and that 13 had been confirmed. The agency said it was working with Congo’s health ministry on a response to the outbreak. The results of tests to determine the specific species of the virus circulating in Ituri are expected within 24 hours, it said in a statement. It is the 17th recorded Ebola outbreak in Congo since the virus was first identified in 1976. Some global health experts said they were alarmed that the first reports of the outbreak emerged so late in its development. “It’s pretty stunning to have first notice of an outbreak in D.R.C., which is very experienced, and have it be so large,” said Jennifer Nuzzo, director of the Pandemic Center at the Brown University School of Public Health. Outbreaks are typically picked up much earlier by the World Health Organization, by the U.S. Centers for Disease Control and Prevention or by news reports, she said. Tedros Ghebreyesus, the director general of the W.H.O., said in a briefing on Friday that the organization was first notified about suspected Ebola cases on May 5 and sent a team to Ituri to investigate. The samples they collected initially tested negative for the virus, he said. Samples were later sent to the National Institute of Biomedical Research in Kinshasa, Congo’s capital, which confirmed on Thursday that some of them had tested positive for Ebola, Dr. Tedros said. Preliminary analyses by the institute in Kinshasa indicate that the virus does not belong to the Zaire species, the only Ebola type for which a licensed vaccine exists. Two other species of Ebola, Sudan and Bundibugyo, had previously been detected in Congo. Dr. Tedros said in a text message that the Ituri samples initially tested negative because the field testing equipment could only detect the Zaire species. Early detection, contact tracing, prompt isolation and care and safe burials are all crucial for containing Ebola outbreaks, the African health agency said. Some of the suspected cases are in Ituri’s main city, Bunia, which could pose a challenge for public health workers, since infectious diseases can spread faster in urban settings. Ebola is transmitted through direct contact with the bodily fluids of an infected person, a fact that often puts people caring for sick family members at risk. In addition, Ituri Province has seen decades of violence linked to insurgent groups. Partly because of that, people frequently cross the borders into Uganda and South Sudan, and back. That could make it harder to trace potential contacts of infected people, as could the prevalence of unregulated mines in one part of Ituri. Guinea, Sierra Leone and Liberia were hit by an Ebola epidemic in 2014 and 2015 that eventually killed more than 11,000 people and sickened more than 28,000 across 10 countries, according to estimates released by the World Health Organization. Responders initially failed to recognize the extent of the outbreak and did not take sufficient steps to prevent its spread. Since then, there has been a string of outbreaks, mainly in Congo and Uganda. But they have been contained, largely because public health officials have reacted quickly, drawing on knowledge and experience gained in past battles with the virus. The Africa Centers for Disease Control and Prevention said it would convene a meeting about the outbreak on Friday that would include health officials from Uganda and South Sudan as well as from the W.H.O. and the U.S. Centers for Disease Control and Prevention. American officials have said that aid cuts by the Trump administration hampered the ability of the authorities in Uganda to curtail an Ebola outbreak in that country early last year. “It’s possible that we’re starting to see the consequences of severe and sudden cuts to global health programs that have eroded surveillance and allowed deadly viruses to spread undetected,” Dr. Nuzzo said.
|
|
Scooped by
Juan Lama
May 13, 12:31 PM
|
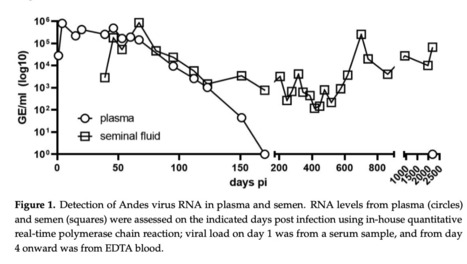
When infecting humans, Andes orthohantavirus (ANDV) may cause a severe disease called hantavirus cardiopulmonary syndrome (HCPS). Following non-specific symptoms, the infection may progress to a syndrome of hemorrhagic fever combined with hyper-acute cardiopulmonary failure. The case fatality rate ranges between 25–40%, depending on the outbreak. In this study, we present the follow-up of a male patient who recovered from HCPS six years ago. We demonstrate that the ANDV genome persists within the reproductive tract for at least 71 months. Genome sequence analysis early and late after infection reveals a low number of mutations (two single nucleotide variants and one deletion), suggesting limited replication activity. We can exclude the integration of the viral genome into the host genome, since the treatment of the specimen with RNAse led to a loss of signal. We demonstrate a long-lasting, strong neutralizing antibody response using pseudovirions expressing the ANDV glycoprotein. Taken together, our results show that ANDV has the potential for sexual transmission. Published in 2023 (Viruses): https://pmc.ncbi.nlm.nih.gov/articles/PMC10675069/
|
|
Scooped by
Juan Lama
May 9, 11:26 AM
|
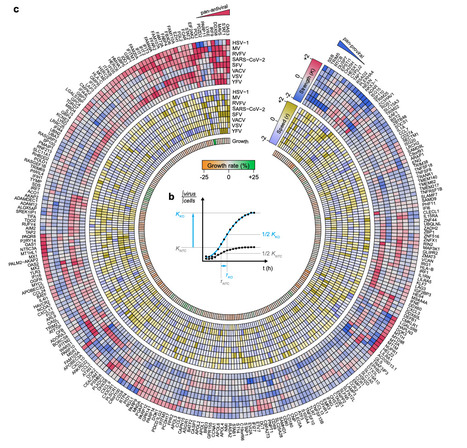
The innate immune system requires the activity of interferon-stimulated genes (ISGs) to mount its protective response against viruses. However, the activity of ISGs against viruses varies widely and is orchestrated by the interplay of hundreds of ISGs. Utilizing a time-resolved, arrayed loss-of-function screen, we systematically investigate 285 ISGs for their virus-modulating activity against eight viruses. The quantitated data from the screen results do not necessarily result in similar quantitative biological effects of gene function but indicates virus specificity of many ISGs and pan-proviral activity of some ISGs, such as RNA 2’,3’-cyclic phosphate and 5’-OH ligase (RTCB). Co-depletions of selected candidates identify ISGs with synergistic functions, highlighting particularly strong synergies between ISGs inhibiting entry pathways and ISGs involved in IFN signaling. Among unexplored ISGs, we identify BORCS8, which has a particularly prominent role in modulating SARS-CoV-2 infection. Mechanistically, BORCS8 mediates the acidification of early endosomes during viral entry, a process known to facilitate the degradation of virus particles. Collectively, this extensive resource reveals specificities of ISGs identified in this screening system and suggests potential strategies for antiviral treatment options. Innate immunity relies on interferon-stimulated genes (ISGs) to restrict viral infection. We identified virus-specific and synergistic actions among 285 ISGs, revealing BORCS8 as a new ISG that limits SARS-CoV-2 by enhancing early endosome acidification. Published in Nat. Comm. ( May 8, 2026): https://www.nature.com/articles/s41467-026-72732-x
|
|
Scooped by
Juan Lama
April 29, 12:35 PM
|
Highlights • Severe IAV infection imparts a long-lasting decline in cardiac function • Atypical GMP-independent CD319+ pro-DC3s transport infectious IAV to cardiomyocytes • Direct IFN-I signaling on cardiomyocytes drives cardiac dysfunction • mod-mRNA delivery of dominant-negative IFNAR1 on cardiomyocytes ameliorates damage Summary Abundant evidence has correlated influenza infection with cardiovascular disease, yet mechanisms linking infection with the heart remain poorly understood. Here, we show that influenza infection damaged the human and murine heart. In mice, we showed that shortly after pulmonary infection, the virus infected a circulating myeloid pro-dendritic cell 3 (pro-DC3) that expressed high concentrations of the chemokine receptor CCR2. The heart, which produces abundant CCL2, preferentially attracted infected pro-DC3. In the myocardium, the virus escaped pro-DC3, infected cardiomyocytes, and triggered production of type-I interferon (IFN-I). Engagement of the IFN-I receptor (IFNAR1) on cardiomyocytes caused tissue damage and compromised heart function. Genetically and therapeutically dampening IFNAR1 exclusively in cardiomyocytes protected the heart while preserving anti-viral immunity in the lung. Our results identify a series of host-pathogen interactions that propagate tissue damage and uncover an axis for intervention to mitigate cardiovascular risk following viral infection. Published in Immunity (March 10, 2026):
|
|
Scooped by
Juan Lama
April 22, 11:48 AM
|
This study investigated stroke incidence after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection using Qatar’s nationwide stroke registry linked with national testing, vaccination, and mortality databases. A self-controlled case series design was implemented among individuals with stroke and confirmed primary SARS-CoV-2 infection between January 1, 2020, and April 11, 2023. Incidence rate ratios (IRRs) comparing stroke incidence rate during the 1–90 days post-infection with predefined control periods were estimated using conditional Poisson regression. Of 4,187 stroke cases, 338 with confirmed infection met inclusion criteria. Stroke incidence rate was elevated during the 1–90 days post-infection (IRR 1.84, 95% CI: 1.31–2.58), peaking at days 1–28 (IRR 2.22, 95% CI: 1.53–3.22) and declining thereafter (days 29–59: IRR 1.47, 95% CI: 0.97–2.24; days 60–90: IRR 0.72, 95% CI: 0.43–1.21). This corresponded to 5.9 excess strokes per 100,000 infections. Elevated risk was confined to pre-Omicron infections (IRR 2.98, 95% CI: 1.89–4.70), with no evidence of increased risk observed for Omicron infections (IRR 0.82, 95% CI: 0.46–1.45). Subtype analyses showed increased risk for ischemic stroke (IRR 1.99, 95% CI: 1.37–2.89) and cerebral venous sinus thrombosis (CVST; IRR 3.52, 95% CI: 1.15–10.78), but not hemorrhagic stroke (IRR 0.64, 95% CI: 0.16–2.51). SARS-CoV-2 infection was associated with a transient elevation in stroke risk, peaking shortly after infection and declining thereafter. Excess risk was confined to pre-Omicron infections and driven primarily by ischemic stroke, while CVST, though rare, showed the strongest relative effect. Published in Scientific Reports (April 2026)
|
|
Scooped by
Juan Lama
April 10, 1:42 PM
|
In 2024, a bovine H5N1 strain was first isolated from dairy cows in Texas and confirmed to transmit cross-species to humans. Therefore, research on treatments for human infection should be accelerated. In our study, the antiviral effects of baloxavir acid (BXA), oseltamivir carboxylate (OSC), EIDD-1931 (NHC), and ribavirin (RBV) against five H5N1 strains were evaluated in vitro. Cell viability and viral replication were measured to assess the antiviral effects. The results showed that the EC50 of BXA treatment was the lowest. The BXA/NHC and BXA/OSC combination treatments showed more potent inhibitory effects than each monotherapy. The 15 mg/kg baloxavir marboxil (BXM) / 125 mg/kg molnupiravir (MNP) and the 15 mg/kg BXM / 10 mg/kg oseltamivir phosphate (OSP) were tested in BALB/c mice. The mice were inoculated with 10 times the 50% mouse lethal dose (10 MLD50) of bovine H5N1 virus. Treatments began 1-day post-infection (1 dpi) and were administered orally twice daily for 5 or 7 days. Changes in body weight, clinical signs, and survival were monitored; lung and brain tissues were collected for virological, immunological, and histological analyses. Most mice died from severe neurological symptoms. Compared with the 5-day treatment, the 7-day treatment effectively inhibited viral replication and increased survival rates to 50% in BXM, BXM/MNP, and BXM/OSP treatments. Mice treated with BXM/MNP or BXM/OSP combination therapy showed lower viral yields in the lungs than those treated with BXM alone. The results provide a reference for human treatment, and extending the 7-day combination treatment should be considered. Published in Emerging Microbes and Infections (March 31, 2026): https://doi.org/10.1080/22221751.2026.2645843
|
|
Scooped by
Juan Lama
April 8, 12:03 PM
|
More than three-quarters of all cases of liver cancer worldwide are associated with chronic viral hepatitis but scientists have been limited in their ability to model how these viruses lead to cancer. In the new study, a Rockefeller team showed that mice infected with an engineered version of a rat virus develop liver inflammation, scarring, and ultimately cancer similar to that seen in humans with viral hepatitis-associated liver cancer. The new mouse model can be used to study how liver virus cause cancer.... Study published in J. Hepatology (March 2026): https://www.journal-of-hepatology.eu/article/S0168-8278(26)00085-1/fulltext
|
|
Scooped by
Juan Lama
March 29, 1:33 PM
|
Many viruses have adapted to persist in infected humans for life1,2. Variable host control of their ongoing abundance (viral load) can lead to clearance or disease3–5. Here we analysed the viral DNA load of 31 common viruses in human blood and saliva using whole-genome sequencing data from UK Biobank (n = 490,401), All of Us (n = 414,817) and Simons Foundation Powering Autism Research for Knowledge (SPARK; n = 12,519). Viral DNA load varied markedly with age, time of day and season; most viruses were also present at greater abundance in men than in women. Human genetic variation at dozens of loci associated with DNA load of seven viruses: Epstein–Barr virus (EBV, 45 loci), human herpesvirus (HHV)-7 (37 loci), HHV-6B, Merkel cell polyomavirus and three anelloviruses. Variation at the major histocompatibility complex (MHC) locus generated the strongest associations (P = 5.8 × 10–9 to 2.5 × 10–1459), which were specific to each virus. The HLA-B*08:01 allele also exhibited a host–virus genetic interaction with EBV subtype (P = 7.4 × 10–70). Other human genetic effects implicated genes encoding proteins that process peptides for antigen presentation, such as ERAP1 (HHV-7, P = 2.7 × 10–78) and ERAP2 (EBV, P = 4.6 × 10–111). Mendelian randomization analyses supported a strong causal effect of EBV DNA load on increased risk of Hodgkin’s lymphoma (P = 1.8 × 10–3), but not multiple sclerosis (P = 0.52). This suggests that higher chronic EBV load increases lymphoma risk, whereas associations of EBV infection with autoimmune conditions reflect host immune responses to particular viral epitopes. Analyses of biobank data show that human variation such as age, sex and genetics, particularly at the major histocompatibility complex locus, is associated with viral abundance and supports a causal link between abundance of Epstein–Barr virus and Hodgkin’s lymphoma. Published in Nature (March 25, 2026): https://doi.org/10.1038/s41586-026-10288-y
|
|
Scooped by
Juan Lama
March 15, 10:53 AM
|
As the U.S. flu season winds down, health officials say the flu vaccine didn’t work very well with one of its worst effectiveness rates in more than a decade. A new strain that dominated the early winter was not well matched to the vaccine, leading to an intense early onslaught of flu. The Centers for Disease Control and Prevention on Friday posted data that showed a continued decline in doctor's office and hospital visits for flu symptoms through last week. The number of states reporting high flu activity dropped to 16, many of them in a belt stretching from Colorado to Virginia. “The winter respiratory virus season is slowly coming to a close, and we’re all very grateful for that,” said Dr. William Schaffner, a Vanderbilt University vaccine expert. This season's vaccines were around 25% to 30% effective in preventing adults from getting sick enough from the flu that they had to go to a doctor’s office, clinic or hospital, according to a CDC report this week. Children who were vaccinated were about 40% less likely to get treatment at a doctor’s office or hospital. Officials generally are pleased if a flu vaccine is 40% to 60% effective. Judging from past CDC research, this season saw one of the lowest effectiveness rates in the last two decades. Flu infections surged in late December and were especially intense in some parts of the country. New York City health officials called it the most intense season in 20 years. Relatively low flu vaccination rates did not help, but experts also blamed the new flu strain that was causing most infections. The new strain belonged to a category of flu virus, called A H3N2. This new version, subclade K, seemed to spread more easily — though it did not necessarily cause more severe illness. The vaccine available for this season was built to address a different version of H3N2, and the new strain's explosion is a likely explanation for why the vaccine was less effective, Schaffner said. CDC scientists estimate there have been at least 27 million illnesses, 350,000 hospitalizations and 22,000 deaths from flu so far this season. At the same point last year, the estimates were at least 40 million illnesses, 520,000 hospitalizations, but about the same number of deaths. At least 101 children have died so far this season. For those whose vaccination status is known, about 85% were not fully vaccinated against flu. The flu vaccine may not protect everyone from getting sick, but it can prevent people from becoming severely ill and dying. That's why getting a flu shot remains worthwhile, Schaffner said. CDC data suggests adult vaccination rates are up slightly this season, to 46.5%, following an unusually bad season last year that set a record for the most child deaths this century. An estimated 48% of U.S. kids were vaccinated against flu around the end of last month. That's about the same as last year, but down from the 52% vaccinated at this point in 2024, according to CDC data. Starting in 2010, the government recommended annual flu vaccinations for Americans 6 months and older. In January, however, the Trump administration stopped broadly recommending flu shots for all children, saying instead that it’s up to parents and family doctors to decide. Meanwhile, work is already underway for next winter’s flu season. Last month, the World Health Organization announced its recommendations for which virus strains to address in the vaccines for the 2026-27 northern hemisphere flu season. The vaccines should be built to handle subclade K, the organization said. This week, a U.S. Food and Drug Administration advisory committee endorsed the WHO recommendations. CDC Report in MMWR (March 12, 2026): https://www.cdc.gov/mmwr/volumes/75/wr/mm7509a2.htm
|
|
Scooped by
Juan Lama
March 12, 12:06 PM
|
Emerging research from the University of Virginia (UVA) has unveiled a startling connection between severe viral respiratory infections and an increased risk for lung cancer development months or even years post-infection. This groundbreaking study, spearheaded by Dr. Jie Sun and colleagues at UVA’s Beirne B. Carter for Immunology Research and Comprehensive Cancer Center, elucidates how severe cases of COVID-19, influenza, and pneumonia induce long-lasting alterations in lung immune cell behavior, effectively “reprogramming” the pulmonary immune landscape to favor tumor growth. Their findings illuminate critical implications for clinical surveillance paradigms, vaccination policies, and future cancer prevention strategies. The investigation began with an acknowledgement of the longstanding gap in understanding the long-term oncogenic consequences of viral lung injuries. Researchers utilized both murine models and retrospective human clinical data to assess how severe respiratory viral infections modulate lung immunity and impact carcinogenesis. Results from murine studies demonstrated that mice afflicted with severe pulmonary infections exhibited a marked propensity to develop lung tumors and suffered higher mortality rates following cancer establishment when compared to uninfected controls. This phenomenon suggested a causative link between intense lung inflammation and an immunological milieu conducive to cancer progression. In parallel analysis, the team accessed large-scale patient datasets revealing a statistically significant association between hospitalization for severe COVID-19 and an elevated incidence of lung cancer, quantified at a 1.24-fold increased risk independent of traditional risk factors like smoking and pre-existing comorbidities. This correlation underscored the real-world clinical relevance of the murine findings and raised urgent questions about post-infection cancer monitoring protocols. Notably, mild COVID-19 cases did not present this increased risk, implying that the severity of immune perturbation is the critical determinant in carcinogenic priming. Mechanistically, the study pinpointed drastic shifts in lung-resident innate immune cells—specifically neutrophils and macrophages—that are ordinarily responsible for pathogen clearance and tissue homeostasis. Following severe viral infection, these cells adopt dysfunctional phenotypes characterized by sustained pro-inflammatory cytokine production and extracellular matrix remodeling. This aberrant activation fosters a chronic inflammatory microenvironment rich in reactive oxygen species and growth factors, creating fertile ground for malignant transformation and tumor growth. Additionally, perturbations to the epithelial lining of alveoli were observed, further compromising the lung’s integrity and enhancing vulnerability to oncogenic insults. A significant and hopeful facet of Sun’s research is the protective effect consistent vaccination confers against these detrimental alterations. Vaccinated individuals, by priming adaptive immunity and curbing viral replication, mitigate the chaotic immune activation and lung injury associated with severe infection. The data suggest that vaccines serve a dual protective role: preventing acute disease hospitalization and abrogating the long-term immune scarring responsible for increased cancer susceptibility. This finding advocates for intensified vaccination efforts not only for infectious disease control but also for cancer prevention in vulnerable populations. The clinical ramifications of these discoveries are profound. Dr. Jeffrey Sturek, a UVA physician-scientist who collaborated on the study, emphasized the need to rethink post-viral infection surveillance akin to long-established cancer risk assessments derived from smoking history. Patients recovering from severe viral pneumonia could benefit from more rigorous and routine lung cancer screening protocols, perhaps integrating low-dose computed tomography scans for early tumor detection. The insights call for personalized medicine approaches that integrate viral infection history into oncological risk stratification models. Beyond clinical implications, the study expands our fundamental understanding of how acute infectious insults can prime chronic disease pathways. It reveals a novel paradigm where immune memory of viral trauma contributes to malignancy, broadening the landscape of cancer etiology beyond genetic and environmental factors. Such knowledge opens avenues for innovative therapeutic interventions aimed at restoring immune cell function and reversing pro-tumor inflammatory imprints in post-infection lungs. UVA’s Beirne B. Carter Center continues to lead in dissecting the complex interplay between infection, immunity, and cancer, building on prior work elucidating immune cell plasticity in disease. The Center’s integrative approach, combining immunology, oncology, and infectious disease expertise, uniquely positions it to translate these findings into targeted therapies. Their efforts are complemented by the UVA Comprehensive Cancer Center’s national leadership in cancer research, recognized through the prestigious National Cancer Institute designation. Publication of this multidisciplinary research in the high-impact journal Cell not only solidifies its scientific rigor but also ensures wide dissemination among the biomedical community. The work was supported by multiple National Institutes of Health grants and UVA institutional awards, highlighting the collaborative investment in addressing pressing health challenges arising from global pandemics and endemic respiratory diseases. Dr. Sun and colleagues stress the urgency for the medical community to incorporate viral infection histories into routine cancer risk evaluation and to champion vaccination as a multifaceted health safeguard. With millions affected worldwide by severe COVID-19 and influenza annually, proactive measures based on this research could markedly reduce lung cancer morbidity and mortality. The authors anticipate that ongoing research will further clarify molecular pathways involved, fostering development of precision medicine interventions to disrupt the cancer-promoting sequelae of viral lung infections. Published in Cell (March 11, 2026): https://www.sciencedirect.com/science/article/abs/pii/S0092867426002205
|
|
|
Scooped by
Juan Lama
June 8, 12:31 PM
|
Traces of HIV-1 RNA can persist in plasma despite long-term suppressive antiretroviral therapy (ART). Some individuals develop nonsuppressible viremia (NSV), characterized by detectable HIV-1 RNA that raises concerns for virological failure, pathogenesis, and transmission. The sources of NSV remain poorly defined, in part due to limited tools to characterize plasma HIV-1 RNA. Both infectious and defective proviruses, including those with defects in the 5′ Leader (5′L), can contribute to NSV, but their relative contributions have not been quantified. Here we show that in over 50 participants, plasma viremia is markedly driven by highly clonal HIV-1 RNA populations carrying defects in the 5′L. Across individuals, dominant clones with 5′L defects clustered around the major splice donor (MSD) accounted for the vast majority of circulating HIV-1 RNA. To enable rapid, scalable profiling, we developed CLAWS (Capturing 5′ Leader Anomalies Without Sequencing), a digital PCR assay that distinguishes intact from defective 5′L RNA. CLAWS recapitulated sequencing-based estimates and detected low-abundance defective RNA early after ART initiation, revealing that defective genomes emerge early and become predominant during long-term therapy. These findings identify 5′L-defective genomes as the predominant driver of NSV and establish CLAWS as a practical tool for monitoring viremia in clinical and cure-related settings. Traces of HIV-1 RNA remain in the plasma despite years of antiretroviral therapy (ART), sometimes causing nonsupressible viremia (NSV). Here, the authors show that 5′Leader-defective RNA is the predominant driver for NSV in ART-treated individuals. Publised in NAt. Comm. (June 8, 2026): https://doi.org/10.1038/s41467-026-73475-5
|
|
Scooped by
Juan Lama
May 27, 1:13 PM
|
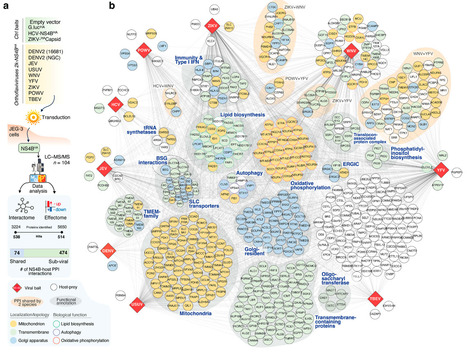
Orthoflavivirus infections represent an increasing public health burden, with several members of the genus emerging or re-emerging globally. Several pre-clinical studies identified the non-structural protein 4B (NS4B), as the most promising target for the development of potent direct-acting antivirals. However, its functional roles in viral replication are still elusive. Here, we employ an integrated proteomic approach to systematically identify cellular targets of NS4B across eight prototypic orthoflaviviruses and characterize their influence on the human proteome. Using this approach, we mapped high-confidence NS4B-interacting human proteins across the genus, underlying potentially divergent and convergent mechanisms of host adaptation across orthoflaviviruses spanning diverse pathologies and vector preferences. Among these, we unveil a novel function for UBA5, the E1-activating enzyme of the UFMylation pathway, in orthoflavivirus replication. Mechanistically, we map associations of distinct viral proteins with multiple members of the UFMylation pathway, which are selectively recruited to sites of viral replication to promote infectious particle production. The study highlights an important requirement of UFMylation for the replication of flaviviruses and the discovery of a novel target for the development of broad anti-flaviviral therapies #flavivirus #DENV #ZIKV #WNVFinally, we demonstrate that pharmacological inhibition of UFMylation exerts potent antiviral activity in vitro and in vivo. This integrative study provides a rational framework for a system-level understanding of orthoflavivirus NS4B effector functions and sheds light on a conserved and unconventional role for UFMylation in orthoflavivirus replication. Here, Rajasekharan et al. identify human targets of the viral NS4B protein across orthoflaviviruses, showing how these viruses hijack the UFMylation pathway to replicate. Blocking this pathway reduced infection in lab and animal models, highlighting a promising antiviral strategy. Published in Nat. Comm. (March 13, 2026): https://doi.org/10.1038/s41467-026-70437-9
|
|
Scooped by
Juan Lama
May 24, 1:25 PM
|
In response to the current Bundibugyo Ebolavirus outbreak in the Democratic Republic of the Congo, the Oxford Vaccine Group (OVG) is working urgently with Oxford’s own Clinical BioManufacturing Facility and the Serum Institute of India Pvt. Ltd. (SIIPL), to rapidly produce and scale doses of our ChAdOx-based monovalent Bundibugyo Ebolavirus candidate vaccine, ChAdOx1 BDBV. At the same time, we are working with our global partners to accelerate the generation of supportive preclinical data for the clinical development and testing of the ChAdOx1 BDBV vaccine in outbreak scenarios, all whilst continuing to follow established scientific, ethical, and regulatory standards. For more than 30 years, researchers at OVG, in the Department of Paediatrics at the University of Oxford, have worked on the development and testing of vaccines against infectious diseases. In response to the 2013–2016 West African Ebola outbreak, OVG and the Jenner Institute led a number of clinical trials testing vaccines against Ebolavirus, including an expedited Phase II clinical trial of an adenovirus/MVA Ebola vaccine regimen, contributing to its approval by the European Medicines Agency in 2020. The research team embedded in these trials have continued developing vaccines against multiple filoviruses, including Sudan Ebolavirus and Marburg virus. During outbreaks in Uganda, Equatorial Guinea and Tanzania between 2022 and 2025, vaccines designed and tested by Professor Teresa Lambe and her team based in OVG and the Pandemic Sciences Institute were selected by the World Health Organization for inclusion in ring vaccination trials, should they have been needed. The ChAdOx platform, a type of viral-vector vaccine, has previously demonstrated a vital role in the development of vaccines for emerging infectious diseases and responding to outbreak scenarios. This platform underpinned the Oxford/AstraZeneca COVID-19 vaccine, which was estimated to have saved more than 6 million lives in its first year of use globally. This long-standing work and existing expertise are critical in enabling a rapid response during public health emergencies. Professor Teresa Lambe OBE, Calleva Head of Vaccine Immunology at the Oxford Vaccine Group and Pandemic Sciences Institute said: 'My hope is that this outbreak can be brought under control quickly and that vaccines are ultimately not needed. Nevertheless, our team and partners will continue working to ensure that potential vaccine options are available if they are needed. 'The ability to move rapidly in situations like this has been built on many years of vaccine research and close collaboration with our global partners.'
|
|
Scooped by
Juan Lama
May 14, 1:13 PM
|
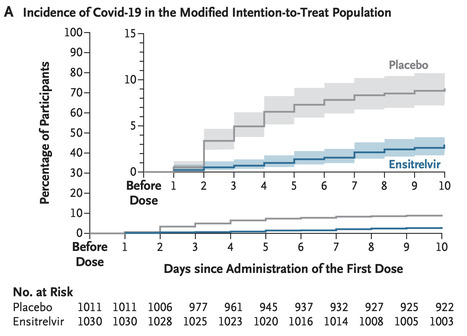
BACKGROUND Ensitrelvir, an oral inhibitor of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) 3C-like protease, is approved in Japan for the treatment of mild-tomoderate coronavirus disease 2019 (Covid-19). Previously, no antiviral agents were approved for postexposure prophylaxis in household contacts of patients with Covid-19. METHODS In this double-blind, randomized, placebo-controlled trial, we randomly assigned persons who were SARS-CoV-2–negative on local diagnostic testing but were household contacts of a patient with Covid-19 (the index patient) to receive either ensitrelvir (375 mg on day 1 and 125 mg daily on days 2 through 5) or placebo within 72 hours after symptom onset in the index patient. The primary end point was Covid-19 (defined by a central laboratory–confirmed positive reverse-transcriptase–polymerase-chain-reaction assay and the presence of ≥1 of 14 prespecified Covid-19 symptoms lasting ≥48 hours) by day 10 in a household contact in the modified intention-to-treat population (all the participants who underwent randomization, had a central laboratory–confirmed negative RT-PCR test for SARS-CoV-2 at baseline, and received at least one dose of the trial drug or placebo). RESULTS The modified intention-to-treat population included 1030 participants in the ensitrelvir group and 1011 in the placebo group. The mean age of the participants was 42.4 years; 71.1% had undergone randomization within 48 hours after symptom onset in the index patient, and 37.0% had at least one risk factor for severe Covid-19. The incidence of Covid-19 was lower in the ensitrelvir group than in the placebo group (2.9% vs. 9.0%; risk ratio, 0.33; 95% confidence interval [CI], 0.22 to 0.49; P<0.001). The incidence of adverse events during the trial was similar in the two groups (15.1% in the ensitrelvir group and 15.5% in the placebo group), as was the incidence of serious adverse events (0.2% in each group). No Covid-19–related hospitalizations or deaths were reported. CONCLUSIONS Ensitrelvir administered to household contacts of a patient with Covid-19 within 72 hours after symptom onset in the index patient was effective in preventing Covid-19 in the contacts. (Funded by Shionogi; SCORPIO-PEP Japan Registry for Clinical Trials number, jRCT2031230124; ClinicalTrials.gov number, NCT05897541.) Published in NEJM (May 13, 2026): https://www.nejm.org/doi/full/10.1056/NEJMoa2509306
|
|
Scooped by
Juan Lama
May 11, 12:09 PM
|
W.H.O. has released interim guidelines for the identification, monitoring, and management of contacts of probable or confirmed Andes virus (ANDV) cases from the MV Hondius cruise ship. The document guides the identification of suspected and probable cases based on symptomatology and relatedness to the hantavirus outbreak. A few highlights - Suggests retesting of symptomatic patients after a negative test as long as they are withing the maximin incubation period (6 weeks).
- Indicates that the period of infectiousness is from onset of symptoms onset until the recovery or death of the case, even though there is no data supporting the lack of infectiousness in asymptomatic patients.
- Defines the date of last contact with a confirmed or probable case (used to guide quarantine) as the date of disembarkation for MV Hondius passengers and crew members
- Classifies different levels of risk for contacts (high and low)
- Provides guidelines to manage and follow contacts, including a 42-day isolation after the last date of contact exposure
Link to the interest guidelines: https://www.who.int/docs/default-source/coronaviruse/situation-reports/who-interim-guidance_management-of-contacts-of-andes-virus-(andv)-cases-from-the-mv-hondius-cruise-ship.pdf
|
|
Scooped by
Juan Lama
April 30, 12:05 PM
|
J. Craig Venter, a scientist and entrepreneur who raced to decode the human genome, died on Wednesday in San Diego. He was 79. His death was announced by the J. Craig Venter Institute, a nonprofit research organization founded by Dr. Venter and based in San Diego and Rockville, Md. The institute said in a statement that Dr. Venter had been hospitalized recently for side effects from cancer treatment. In the 1990s, Dr. Venter, a risk-taker and intense competitor, made a bold move when he decided that the Human Genome Project, a $3 billion government program for decoding the human genome, was moving slowly enough that he could enter the race late and beat it with a much faster method. His gamble paid off. In 2000, his company, Celera, made a joint announcement with a rival group saying that they had assembled the first human genomes, a landmark step toward uncovering the genetic basis of human disease and origins. Dr. Venter had a powerful ego. That was clear when he let slip that the anonymous donor whose genome Celera had sequenced was none other than his own. But his drive and management skills helped him inspire loyalty and assemble teams of exceptional scientists, including the Nobel Prize-winning microbiologist Hamilton O. Smith. Together, they achieved one landmark after another in the nascent field of genomics. In 1995, Dr. Venter revolutionized microbiology when he published the sequence of DNA letters in the bacterium Haemophilus influenzae, the first bacterial genome to be decoded, along with annotations of all the organism’s genes. The moment electrified science. For the first time, researchers could see all the genetic components of a free-living organism, giving microbiologists a manual for bacterium’s genetic tool kit. It also set off a race to sequence the genomes of known pathogens, with the aim of identifying their genetic arsenals and devising countermeasures. His team next turned to the fruit fly genome to test whether their approach, known as a whole-genome shotgun sequencing, could work on its biggest target: the human genome. The fruit fly genome was successfully decoded in 2000, providing a wealth of information that would help scientists study both the fly and human genomes. Decoding the human genome, Dr. Venter’s next big challenge, became the focus of a competition between his team at Celera against a consortium of academic rivals led by the United States and Britain. The National Institutes of Health, a major patron of the effort, refused to cooperate with Dr. Venter, who instead secured private funding from the Celera Corporation. Dr. Venter’s whole genome shotgun method enabled him to erase his rivals’ head start. With ample time and money, he might have seized this greatest of scientific prizes. Instead, he agreed, reluctantly, to accept the consortium’s offer of a formal draw, with the trappings of a White House ceremony with President Bill Clinton. For his contributions to sequencing the human genome, Dr. Venter received the Nierenberg Prize for Science in the Public Interest from the Scripps Institution of Oceanography in 2007. President Barack Obama presented him with the National Medal of Science in 2009.
|
|
Scooped by
Juan Lama
April 24, 12:04 AM
|
The Food and Drug Administration on Thursday approved Regeneron’s Otarmeni, the first gene therapy for genetic hearing loss. The drugmaker said it will offer the drug for free to U.S. patients. Otarmeni is approved to treat a very rare form of hearing loss that affects about 50 babies born in the U.S. each year and is caused by a mutation in a gene called OTOF. The approval was granted under the Commissioner’s National Priority Voucher, an FDA pilot program intended to fast-track drug reviews. “This really is life-changing for families with children with hearing loss,” Dr. Eliot Shearer, a pediatric otolaryngologist at Boston Children’s Hospital and a principal investigator on the Regeneron trial. The only other treatment option for children with genetic deafness is cochlear implants, Shearer said, which restore the ability to hear speech and music, but reduce the fidelity of the sound.With gene therapy, the improved hearing is “on 24/7 and doesn’t rely on batteries,” he added. The drug works by replacing the faulty OTOF gene, which is supposed to work by giving the body instructions to make a protein called otoferlin. This protein plays a role in transmitting pulses from cochlear cells within the ear to nearby nerves, which carry the signals on to the brain. Without otoferlin, sound never reaches the brain. Thursday’s approval was based on a trial of 20 children diagnosed with the OTOF mutation who got a single dose of the therapy in one or both ears. The trial found that it improved hearing in 16 of the 20 children, with five kids developing the ability to detect whispers. Side effects included infection or inflammation of the middle ear, vomiting, nausea and dizziness. The approval was touted by President Donald Trump during an Oval Office announcement Thursday afternoon about a drug pricing deal with Regeneron to provide many of its drugs at a discount on the self-pay platform TrumpRx. While the company is providing the drug at no cost, it has no say over the cost of administering the drug. Shearer said the procedure is similar to surgery for cochlear implants, where doctors access the inner ear to deliver the drug while the patient is under general anesthesia. The drug is not approved outside the U.S., so Regeneron does not have a list price for people abroad who want to get the treatment. Gene therapy prices can be in the millions. Sarah Emond, president and CEO of the Institute for Clinical and Economic Review, a nonprofit group that evaluates the cost and effectiveness of drugs, said Regeneron should be commended on its pricing. “Regeneron has shown us that one option we can consider that will ensure affordable access for patients to these therapies is to not charge the health system for the therapy,” Emond said.
|
|
Scooped by
Juan Lama
April 17, 1:44 PM
|
A study conducted at the University of São Paulo (USP) in Brazil reveals that tissues such as the tonsils and adenoids can serve as hiding places for the rhinovirus, which causes the common cold and is responsible for most respiratory infections worldwide. Using samples from 293 children who underwent surgery to remove these tissues, the study showed that the pathogen can infect immune cells known as lymphocytes and remain there for long periods without causing symptoms. This allows the virus to potentially be transmitted to others without warning. The findings are published in the Journal of Medical Virology. "The virus has a 'date' with the child population. Every year, about two or three weeks after school starts in temperate regions, there's a rhinovirus outbreak. And children pass it on to their parents and grandparents. We've always wondered: What does the start of school have to do with it? Well, children gather in closed spaces, and some of them with the virus in their throats can spark an outbreak at school, even if they're asymptomatic," comments rhinovirologist Eurico de Arruda Neto, a professor at the Ribeirão Preto School of Medicine (FMRP-USP) and coordinator of the research. As the researcher explains, it was already known that the rhinovirus infects the epithelium (the outermost layer of the mucosa) of the nose and throat, hijacks the cellular machinery to multiply, and causes the host cell to rupture once this process is complete, releasing progeny capable of generating new infections. For this reason, scientists consider it a lytic virus, one that causes cell lysis (rupture). This rapid and destructive cycle quickly draws the attention of the immune system, which, in most cases, eliminates the virus from the body within about five to seven days. The major finding of the study was that the rhinovirus can reach the deeper layers of tonsil and adenoid tissues in addition to the epithelium. There, it can infect B lymphocytes, which produce antibodies, and CD4 T lymphocytes, which conduct the local immune response. These cells have a long lifespan and store the "memory" of the immune system. Rather than killing them, the rhinovirus remains inside these cells for extended periods, in a state of persistence similar to that seen with herpes viruses, HPV, and cytomegalovirus. "The samples we analyzed are from children who underwent surgery due to snoring, sleep apnea, or recurrent infections related to tonsillar and adenoid hypertrophy. At the time of surgery, they were necessarily asymptomatic. Nevertheless, we detected the rhinovirus in a large number of participants," says Arruda. In addition to the tonsils and adenoids, the children's nasal secretions were analyzed as well. According to the study, the virus was present in at least one of the three sites (tonsil, adenoid, or secretion) in 46% of the volunteers. Viral proteins and other signs that the rhinovirus was replicating—and therefore capable of infecting another person—were also observed in these tissues. The research was conducted in collaboration with Ronaldo Martins, a virologist from the Ribeirão Preto School of Pharmaceutical Sciences (FCFRP-USP), as well as professors Wilma Anselmo-Lima, Edwin Tamashiro, and Fabiana Valera from the FMRP-USP. 'Virus garden' In previous studies, Arruda's team had detected adenovirus (another cause of the common cold), influenza A (flu), and SARS-CoV-2 (COVID-19) in samples of tonsils and adenoids from children who had undergone surgery. The latter two are known to cause longer-lasting infections in some patients. In the case of the rhinovirus, however, this came as a surprise. "I get the impression that no matter what common virus we look for, we'll find it. And not just in the tonsils and adenoids, but in other lymphoid tissues throughout the body, such as lymph nodes. We already have some preliminary evidence that lymphoid tissues are a sort of 'garden' for viruses. And our hypothesis is that this is a good thing. It acts as a booster for immune memory, meaning antibodies continue to be produced even long after initial exposure," says Arruda. However, in the case of people with asthma, this can be problematic. One hypothesis raised by the authors of the article is that infectious viruses in tonsil CD4 T lymphocytes may release inflammatory substances that act on the lungs and cause asthma attacks. It is already known that colds and the flu are among the most common causes of asthma attacks, especially in young children. Additionally, a previous study by the group detected respiratory viruses in normal adenoids (without hypertrophy), which are located next to the Eustachian tube. This may explain why some children suffer from recurrent otitis media. "This virus can pass from the adenoids to the middle ear and cause inflammation there. The child won't sneeze or cough, but the ear will become inflamed, closing the narrow Eustachian tube and leading to a buildup of fluid in which the local bacterial flora begins to proliferate," the researcher explains. Clinical implications Based on these findings, Arruda believes that pediatricians should be mindful of the possibility of diagnostic confusion regarding the causes of childhood illnesses. "For example, a child with hypertrophic tonsils arrives at the emergency room with a respiratory infection and bronchiolitis symptoms caused by respiratory syncytial virus, but the throat swab test detects rhinovirus from a previous infection. In other words, tests performed on secretions may not always reflect what's actually happening in the lungs," says the researcher. "We have evidence that this viral persistence can also occur in people with normal-sized tonsils and adenoids." Another hypothesis to be investigated, Arruda says, is whether viruses that persist in lymphoid tissues can cause problems for immunosuppressed patients. "Patients who undergo bone marrow transplants, for example, frequently develop lung infections and bronchiolitis. Doctors, nurses, and medical students are usually blamed for bringing the virus into the high-risk ward. But could it be that the virus was already present in the patient's tonsils or adenoids and has now been reactivated due to low immunity? It doesn't have to be transmission from outside to inside. That's what we've started to investigate in mice," he explains. Study published Jan. 2026: https://onlinelibrary.wiley.com/doi/10.1002/jmv.70809
|
|
Scooped by
Juan Lama
April 10, 1:19 PM
|
The acting director of the Centers for Disease Control and Prevention has delayed publication of a CDC report showing the covid-19 vaccine cut the likelihood of emergency department visits and hospitalizations for healthy adults last winter by about half, according to two scientists familiar with the decision. The scientists spoke on the condition of anonymity for fear of retaliation. The move has raised concerns among current and former officials that information about the vaccine’s benefits are being downplayed because they conflict with the views of Health Secretary Robert F. Kennedy Jr., who has been an outspoken critic of the shots. The delay, which has not been previously reported, offers a window into how vaccine policy is being shaped behind the scenes, even as the Trump administration has sought to soften its public posture on controversial actions ahead of the midterm elections. The report had been scheduled for publication March 19 in the CDC’s flagship scientific journal, the Morbidity and Mortality Weekly Report, the scientists said. Between September and December last year, healthy adults who received the vaccine reduced their likelihood of emergency department and urgent care visits by 50 percent and cut the likelihood of covid-associated hospitalizations by 55 percent, compared with those not receiving a 2025-2026 vaccine dose, according to a summary of the report obtained by The Washington Post. The report had cleared the agency’s scientific-review process, the scientists said, but now it has been delayed by acting CDC director Jay Bhattacharya over concerns about the methodology, the scientists said. The same methodology has long been used by the CDC to evaluate vaccine effectiveness for respiratory viruses, including influenza. A report about flu vaccine effectiveness this past winter — using the same methodology — was published in the MMWR a week earlier. That methodology was also used in a 2021 study on covid vaccine effectiveness in clinics and hospitals published in the New England Journal of Medicine. Vaccine effectiveness estimates using the same methodology have also been published in other peer-reviewed journals, including JAMA Network Open, the Lancet and Pediatrics....
|
|
Scooped by
Juan Lama
April 3, 12:31 PM
|
AI predicted that a forgotten breast cancer drug could be repurposed to treat many respiratory and gastrointestinal viruses, and subsequent animal tests suggests it may be right. A single drug has been found to inhibit a range of common viruses in lab studies, including coronaviruses, respiratory syncytial virus (RSV), norovirus, and influenza and hepatitis viruses. It will be tested in a clinical trial next year, raising hopes that the pill could one day be taken at home to relieve unpleasant symptoms or even limit infections if there were another viral pandemic. “As far as we can tell, this is the first drug that’s ever demonstrated activity across all these viral families,” says Daniel Haders, co-founder of Model Medicines, the California-based company leading its development. If it is approved, Haders envisages it being a pill that people could take if, for example, they have a flu-like illness but don’t know if it is influenza, covid-19, RSV or something else...
|
|
Scooped by
Juan Lama
March 26, 12:39 PM
|
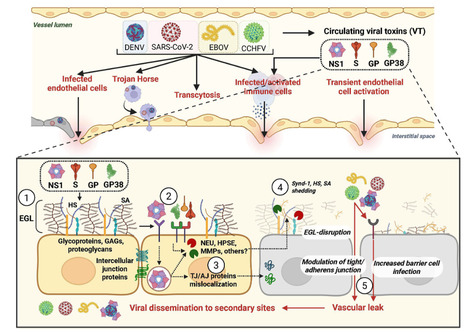
The process by which viruses cause disease, viral pathogenesis, is the result of both infection of cells and the host immune response. A less studied but equally important contributor to viral pathogenesis is viral dissemination, the capacity of a virus to move from the primary site of infection, traverse physiological barriers, and gain access to secondary sites of infection. This dictates viral tropism and pathogenesis, but the mechanisms governing barrier crossing are incompletely understood. While the presence of viral receptors on cells is a major determinant of viral tropism and a prerequisite for infection, it does not completely explain the capacity of viruses to enter a tissue. Our recent work has begun to characterize the contribution of soluble viral proteins, acting as “viral toxins,” to viral dissemination, tissue tropism, and overall pathogenesis within an infected host. In this review, we discuss the characteristics of these viral toxins, which are soluble or surface-exposed viral proteins that can interact with endothelial and/or epithelial barriers, as well as immune cells, to trigger signaling pathways, resulting in the transient breakdown of cellular structures maintaining barrier integrity. The disruption of these barriers induces vascular leak and facilitates virus dissemination, influencing viral tropism and pathogenesis. Importantly, blocking this process prevents leak, viral dissemination, and severe disease during infection, highlighting the value of therapeutic intervention against viral toxin activity. Here, we summarize our current understanding of recently discovered viral toxins from the Flaviviridae, Coronaviridae, Nairoviridae, and Filoviridae. Published March 13, 2026 in MBio:
|
|
Scooped by
Juan Lama
March 14, 12:26 PM
|
Evidence suggests reactivations of the varicella-zoster virus may accelerate aging and raise dementia risk. Now scientists want to know if vaccines and antivirals could help protect the brain. The lecturer—a 63-year-old viral immunologist whose identity has been kept anonymous—suffered alarming symptoms, including impaired memory, waning concentration, and difficulty reading. While giving lectures to students, he found he had difficulty focusing and was often unable to finish sentences without pausing. But medical tests, including a brain biopsy, failed to get to the source of the problem, and over the next four years, his symptoms continued to progress. His decline would have likely continued unabated had he not heard about a case of encephalitis—serious brain inflammation caused by a reactivation of the varicella-zoster virus, most commonly associated with childhood chickenpox and, later in life, shingles. Remembering that his own symptoms had been preceded by a brief case of shingles, subsequent tests confirmed the patient had indeed experienced a reactivation of varicella-zoster. And so he decided to treat the problem with a course of acyclovir, an antiviral drug commonly prescribed to shingles patients. To his colleagues’ amazement, the Colorado lecturer’s symptoms quickly faded away and his cognition returned to normal. This remarkable case study, published in 2016, has inspired neurovirologists to look deeper into the connection between shingles and brain aging. For decades, shingles has been predominantly associated with a form of nerve pain known as postherpetic neuralgia, which can be so severe that it was once cited as the leading cause of pain-related suicide in the elderly. Now, research is starting to reveal the devastating impact that shingles can have on brain health. According to Andrew Bubak, assistant professor of neurology at the University of Colorado Anschutz, the true burden of varicella-zoster “is totally underestimated. But it’s a very treatable virus.” In recent years, increasing numbers of studies have shown that the shingles vaccine appears to be capable of protecting the aging body and brain, and dementia specialists are taking note. In April 2025, a major study by researchers at Stanford University suggested vaccination against shingles could prevent one in five new cases of dementia. More recent studies have also linked getting a shingles vaccine to slower biological aging across a variety of measures. One explanation given for the findings is that the vaccine might be stimulating the immune system in a broadly beneficial manner. While there is likely some truth in this, additional research increasingly points to the value of avoiding shingles (or reactivations of the varicella-zoster virus) in the first place, with two separate studies finding associations between shingles and self-reported cognitive decline and dementia. Neurovirologists believe this emerging data underlines the importance of avoiding infection, through the childhood chickenpox vaccination—given to children in the US since 1995 and introduced in the UK in January 2026—and through the adult shingles vaccine and booster jabs in later life. Before the US started routinely vaccinating against chickenpox, more than 90 percent of children acquired the varicella-zoster virus in childhood. Following the infection, the virus takes up position in the peripheral nervous system—the neurons linking the brain and spinal cord to the limbs and organs—where it stays dormant, sometimes for decades. Varicella-zoster can reactivate in the body following various triggers, which range from acute stress to concussion, co-infections with Covid-19, immunosuppressive medications, and the general aging of the immune system. In many cases, such reactivations may be completely symptomless, with some studies suggesting many of us could unknowingly experience repeated “subclinical” reactivations—the virus reawakening from its dormant state without inducing visible symptoms—in mid- to later life. “We rely on specialized immune cells to continuously patrol the nervous system and keep the dormant virus suppressed,” says Tian-Shin Yeh, associate professor of medicine at Taipei Medical University and attending physician at Shuang Ho Hospital in Taiwan. “As we get older, these cells can become less effective, or exhausted.” Once varicella-zoster reactivates, several things can take place. The virus is part of the herpes family, members of which are particularly adept at infiltrating the brain and central nervous system due to their ability to exploit its internal transport mechanisms for their own use. “Our nerve cells contain molecular motors that shuttle cargo along the nerve fibers,” says Yeh. “Herpes viruses can commandeer these transport systems to move from peripheral tissues deep into the nervous system.”....
|
|
Scooped by
Juan Lama
February 23, 11:16 AM
|
An innovative approach supercharges the innate immune system to provide a first line of defence against respiratory infections. Imagine if a nasal spray could make you immune not only to the viruses that cause COVID-19 and influenza, but to all respiratory diseases. In a paper1 published in Science today, researchers describe a vaccine that has done just that. When given to mice, the vaccine protected them for at least three months against multiple disease-causing viruses and bacteria — including the SARS-CoV-2 virus that causes COVID-19 — and even quelling responses to respiratory allergens. If the research translates to humans safely and effectively, such a ‘universal vaccine’ could be offered to everyone at the start of each winter — and perhaps provide a first line of defence against future pandemics. Bali Pulendran, an immunologist at Stanford University in Palo Alto, California, and his group previously studied the Bacillus Calmette–Guérin (BCG) vaccine2, which provides temporary protection against numerous diseases and works by activating the innate immune system and keeping it active. This evolutionarily ancient system has a much broader reactivity than does the adaptive immune system — which is the one conventional vaccines utilize by teaching antibody-making B cells and T cells to recognize proteins found on specific pathogens. Activating the innate immune system can also induce the intrinsic capacity of the respiratory system’s epithelial cells to resist infection. These cells are the target of many pathogens. Double bulwark In the latest study, Pulendran’s team developed a universal vaccine that targets the innate immune system, with three components. The first two are drugs that stimulate specific receptor proteins that can activate innate immune cells, such as macrophages that reside in the lungs. The third component stimulates a population of T cells, which are part of the adaptive immune system. Their task is to keep sending signals to the innate immune system to maintain its active state. The vaccine contains an immunogenic protein from chicken eggs, and in experiments in which it was omitted, immunity quickly waned. Mice that were given four doses of the nasally delivered vaccine developed immunity to SARS-CoV-2 and other coronaviruses, plus to bacteria that cause certain respiratory infections. Another novel benefit was that the activated pathways also suppressed the mechanisms that mediate hypersensitivity to house dust mites, thereby preventing allergic asthma. Analyses of how the protection works revealed what Pulendran calls a two-bulwark system, in which an initial mucosal barrier limits pathogen entry into the lungs. “Then,” he says, “this mucosal vaccination has set up the lung immune system, so that it is extraordinarily rapid in eliciting the virus-specific immune response to send off those few viruses that slip through the initial bulwark.” Bridge vaccine “It’s really a fantastic paper, and it’s exciting. The data look very clear to me,” says Akiko Iwasaki, an immunobiologist at Yale University in New Haven, Connecticut. “If it works in humans, that would be really quite remarkable.” Zhou Xing, an immunologist at McMaster University in Hamilton, Canada, says that people who are familiar with the advances in mucosal vaccines over the last decade will not be surprised by the findings. “We call it a ‘bridge vaccine’,” he says — the idea of leveraging the innate immune system to generate non-selective pathogen protection. Both Xing and Iwasaki warn that translating the effectiveness seen in mice into clinical therapies for people isn’t straightforward. Xing fears that without advanced aerosol delivery methods, a nasally delivered vaccine in humans won’t reach the lungs to activate the immune pathways described here. (The small size of mice means that both nasal sprays and pathogens can easily access their lungs.) Xing also says that roll out of the vaccine on a large scale could prove impractical if people need four doses. Because this approach puts the immune system in a state of constant hypervigilance, it could also come with potential side effects. “The cost–benefit ratio is something that one has to assess very, very cautiously in humans,” Pulendran says. If no problems are encountered in an initial, dose-escalation safety trial, a second trial would then use controlled infections, he predicts. That is, sometime after vaccination, healthy volunteers would be deliberately exposed to the influenza virus, for example, to see if they are protected.If they are, a new form of preventive medicine might be in the offing. “Mice provide you with the conceptual framework and evidence of how it could work,” Pulendran says. “But really, the proof of the pudding is: does it really work in humans?” Study published in Science (feb. 19, 2026): https://www.science.org/doi/10.1126/science.aea1260
|