Your new post is loading...

|
Scooped by
HAS-veille
September 26, 2023 2:12 AM
|
|
|
Scooped by
HAS-veille
September 19, 2023 9:47 AM
|
|
|
Scooped by
HAS-veille
September 15, 2023 6:55 AM
|
We have recently demonstrated a causal link between loss of gonadotropin-releasing hormone (GnRH), the master molecule regulating reproduction, and co…
|
|
Scooped by
HAS-veille
September 5, 2023 2:43 AM
|
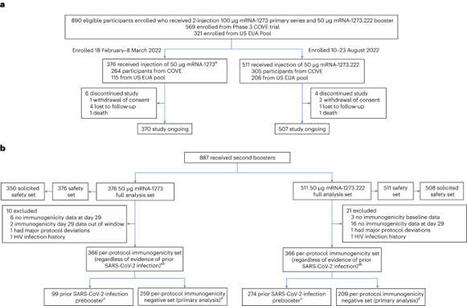
This ongoing, open-label, phase 2/3 trial compared the safety and immunogenicity of the Omicron BA.4/BA.5-containing bivalent mRNA-1273.222 vaccine with the ancestral Wuhan-Hu-1 mRNA-1273 as booster doses. Two groups of adults who previously received mRNA-1273 as primary vaccination series and booster doses were enrolled in a sequential, nonrandomized manner and received single-second boosters of mRNA-1273 (n = 376) or bivalent mRNA-1273.222 (n = 511). Primary objectives were safety and the noninferiority or superiority of neutralizing antibody (nAb) responses against Omicron BA.4/BA.5 and ancestral SARS-CoV-2 with the D614G mutation (ancestral SARS-CoV-2 (D614G)), 28 days post boost. Superiority and noninferiority were based on prespecified success criteria (lower bounds of 95% CI > 1 and < 0.677, respectively) of the mRNA-1273.222:mRNA-1273 geometric mean ratios. Bivalent Omicron BA.4/BA.5-containing mRNA-1273.222 elicited superior nAb responses against BA.4/BA.5 versus mRNA-1273 and noninferior responses against ancestral SARS-CoV-2 (D614G) at day 29 post boost in participants without detectable prior SARS-CoV-2 infection. Day 29 seroresponses against Omicron BA.4/BA.5 were higher for mRNA-1273.222 than for mRNA-1273 and similar against ancestral SARS-CoV-2 (D614G), both meeting noninferiority criterion. The safety profile of mRNA-1273.222 was similar to that previously reported for mRNA-1273 with no new safety concerns identified. Continued monitoring of neutralization and real-world vaccine effectiveness are needed as additional divergent-virus variants emerge. ClinicalTrials.gov registration: NCT04927065. An Omicron BA.4/BA.5 mRNA booster vaccine elicits high neutralizing responses to the BA.4/BA.5 variant and to ancestral SARS-CoV-2, supporting tailoring booster vaccines to the predominant Omicron variant.
|
|
Scooped by
HAS-veille
September 1, 2023 8:56 AM
|
|
|
Scooped by
HAS-veille
August 31, 2023 6:55 AM
|
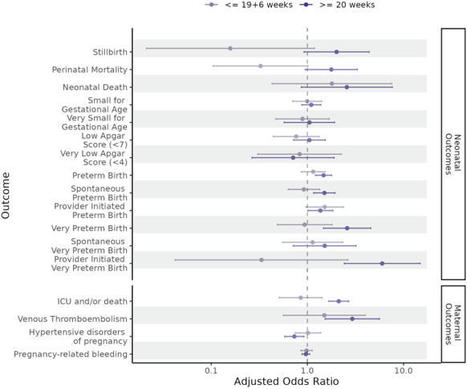
Understanding the impact of SARS-CoV-2 infection and COVID-19 vaccination in pregnancy on neonatal and maternal outcomes informs clinical decision-making. Here we report a national, population-based, matched cohort study to investigate associations between SARS-CoV-2 infection and, separately, COVID-19 vaccination just before or during pregnancy and the risk of adverse neonatal and maternal outcomes among women in Scotland with a singleton pregnancy ending at ≥20 weeks gestation. Neonatal outcomes are stillbirth, neonatal death, extended perinatal mortality, preterm birth (overall, spontaneous, and provider-initiated), small-for-gestational age, and low Apgar score. Maternal outcomes are admission to critical care or death, venous thromboembolism, hypertensive disorders of pregnancy, and pregnancy-related bleeding. We use conditional logistic regression to derive odds ratios adjusted for socio-demographic and clinical characteristics (aORs). We find that infection is associated with an increased risk of preterm (aOR=1.36, 95% Confidence Interval [CI] = 1.16–1.59) and very preterm birth (aOR = 1.90, 95% CI 1.20–3.02), maternal admission to critical care or death (aOR=1.72, 95% CI = 1.39–2.12), and venous thromboembolism (aOR = 2.53, 95% CI = 1.47–4.35). We find no evidence of increased risk for any of our outcomes following vaccination. These data suggest SARS-CoV-2 infection during pregnancy is associated with adverse neonatal and maternal outcomes, and COVID-19 vaccination remains a safe way for pregnant women to protect themselves and their babies against infection. The impacts of SARS-CoV-2 infection and COVID-19 vaccination in pregnancy are not fully understood. Here, the authors perform a cohort study using data from Scotland and find that infection was associated with increased risk of preterm birth and some adverse maternal outcomes, but there was no evidence of adverse outcomes associated with vaccination.
|
|
Scooped by
HAS-veille
August 30, 2023 5:59 AM
|
Our findings suggest that PCS can persist beyond 20 months post-infection and encompass
the full scope of post-infectious ME/CFS as defined by the CCC. Sub-classifying patients
with PCS based on the CCC can assist in the management and monitoring of patients
with PCS-ME/CFS due to their persistently higher symptom severity.
|
|
Scooped by
HAS-veille
August 29, 2023 1:56 AM
|
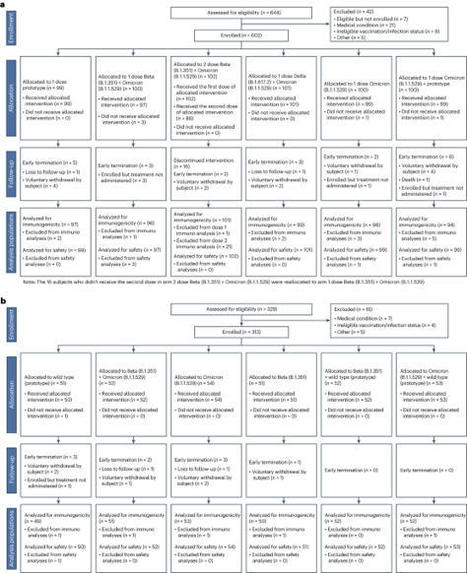
Vaccine protection against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection wanes over time, requiring updated boosters. In a phase 2, open-label, randomized clinical trial with sequentially enrolled stages at 22 US sites, we assessed safety and immunogenicity of a second boost with monovalent or bivalent variant vaccines from mRNA and protein-based platforms targeting wild-type, Beta, Delta and Omicron BA.1 spike antigens. The primary outcome was pseudovirus neutralization titers at 50% inhibitory dilution (ID50 titers) with 95% confidence intervals against different SARS-CoV-2 strains. The secondary outcome assessed safety by solicited local and systemic adverse events (AEs), unsolicited AEs, serious AEs and AEs of special interest. Boosting with prototype/wild-type vaccines produced numerically lower ID50 titers than any variant-containing vaccine against all variants. Conversely, boosting with a variant vaccine excluding prototype was not associated with decreased neutralization against D614G. Omicron BA.1 or Beta monovalent vaccines were nearly equivalent to Omicron BA.1 + prototype or Beta + prototype bivalent vaccines for neutralization of Beta, Omicron BA.1 and Omicron BA.4/5, although they were lower for contemporaneous Omicron subvariants. Safety was similar across arms and stages and comparable to previous reports. Our study shows that updated vaccines targeting Beta or Omicron BA.1 provide broadly crossprotective neutralizing antibody responses against diverse SARS-CoV-2 variants without sacrificing immunity to the ancestral strain. ClinicalTrials.gov registration: NCT05289037 . Analysis of antibody responses to COVID-19 vaccines encoding variant-specific spike, with or without ancestral spike, suggests no loss of neutralization of the ancestral virus with variant-only vaccines, which may simplify future vaccine updates.
|
|
Scooped by
HAS-veille
August 24, 2023 8:25 AM
|
|
|
Scooped by
HAS-veille
August 22, 2023 7:59 AM
|
COVID-19 severity is associated with its respiratory manifestations. Neutralising antibodies against SARS-CoV-2 administered systemically have shown c…
|
|
Scooped by
HAS-veille
August 22, 2023 2:48 AM
|
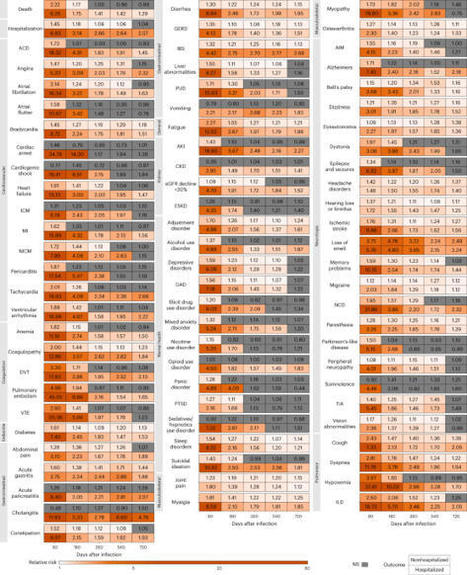
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can lead to postacute sequelae in multiple organ systems, but evidence is mostly limited to the first year postinfection. We built a cohort of 138,818 individuals with SARS-CoV-2 infection and 5,985,227 noninfected control group from the US Department of Veterans Affairs and followed them for 2 years to estimate the risks of death and 80 prespecified postacute sequelae of COVID-19 (PASC) according to care setting during the acute phase of infection. The increased risk of death was not significant beyond 6 months after infection among nonhospitalized but remained significantly elevated through the 2 years in hospitalized individuals. Within the 80 prespecified sequelae, 69% and 35% of them became not significant at 2 years after infection among nonhospitalized and hospitalized individuals, respectively. Cumulatively at 2 years, PASC contributed 80.4 (95% confidence interval (CI): 71.6–89.6) and 642.8 (95% CI: 596.9–689.3) disability-adjusted life years (DALYs) per 1,000 persons among nonhospitalized and hospitalized individuals; 25.3% (18.9–31.0%) and 21.3% (18.2–24.5%) of the cumulative 2-year DALYs in nonhospitalized and hospitalized were from the second year. In sum, while risks of many sequelae declined 2 years after infection, the substantial cumulative burden of health loss due to PASC calls for attention to the care needs of people with long-term health effects due to SARS-CoV-2 infection. Analysis of data from the US Department of Veterans Affairs showed that 2 years after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, risk for most postacute sequelae remained elevated in people who were hospitalized with COVID-19 but was attenuated in nonhospitalized individuals.
|
|
Scooped by
HAS-veille
August 10, 2023 4:09 AM
|
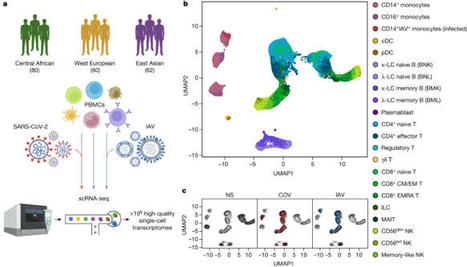
Humans display substantial interindividual clinical variability after SARS-CoV-2 infection1–3, the genetic and immunological basis of which has begun to be deciphered4. However, the extent and drivers of population differences in immune responses to SARS-CoV-2 remain unclear. Here we report single-cell RNA-sequencing data for peripheral blood mononuclear cells—from 222 healthy donors of diverse ancestries—that were stimulated with SARS-CoV-2 or influenza A virus. We show that SARS-CoV-2 induces weaker, but more heterogeneous, interferon-stimulated gene activity compared with influenza A virus, and a unique pro-inflammatory signature in myeloid cells. Transcriptional responses to viruses display marked population differences, primarily driven by changes in cell abundance including increased lymphoid differentiation associated with latent cytomegalovirus infection. Expression quantitative trait loci and mediation analyses reveal a broad effect of cell composition on population disparities in immune responses, with genetic variants exerting a strong effect on specific loci. Furthermore, we show that natural selection has increased population differences in immune responses, particularly for variants associated with SARS-CoV-2 response in East Asians, and document the cellular and molecular mechanisms by which Neanderthal introgression has altered immune functions, such as the response of myeloid cells to viruses. Finally, colocalization and transcriptome-wide association analyses reveal an overlap between the genetic basis of immune responses to SARS-CoV-2 and COVID-19 severity, providing insights into the factors contributing to current disparities in COVID-19 risk. Population differences in immune responses to SARS-CoV-2 can be explained by environmental exposures, but also by local adaptation acting through genetic variants acquired after admixture with archaic hominin forms.
|
|
Scooped by
HAS-veille
August 9, 2023 4:25 AM
|
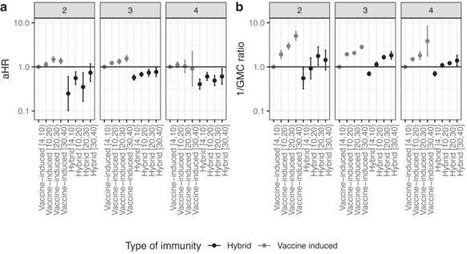
An increasing proportion of the population has acquired immunity through COVID-19 vaccination and previous SARS-CoV-2 infection, i.e., hybrid immunity, possibly affecting the risk of new infection. We aim to estimate the protective effect of previous infections and vaccinations on SARS-CoV-2 Omicron infection, using data from 43,257 adult participants in a prospective community-based cohort study in the Netherlands, collected between 10 January 2022 and 1 September 2022. Our results show that, for participants with 2, 3 or 4 prior immunizing events (vaccination or previous infection), hybrid immunity is more protective against infection with SARS-CoV-2 Omicron than vaccine-induced immunity, up to at least 30 weeks after the last immunizing event. Differences in risk of infection are partly explained by differences in anti-Spike RBD (S) antibody concentration, which is associated with risk of infection in a dose-response manner. Among participants with hybrid immunity, with one previous pre-Omicron infection, we do not observe a relevant difference in risk of Omicron infection by sequence of vaccination(s) and infection. Additional immunizing events increase the protection against infection, but not above the level of the first weeks after the previous event. The relative protection against Omicron SARS-CoV-2 infection conferred by vaccination and previous infection are not fully understood. Here, the authors use data from a prospective cohort study in the Netherlands and show that hybrid immunity (vaccination plus previous infection) conferred strongest protection.
|
|
|
Scooped by
HAS-veille
September 20, 2023 10:26 AM
|
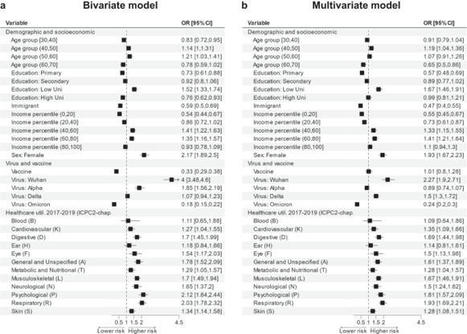
Whereas the nature of the post-COVID condition following mild acute COVID-19 is increasingly well described in the literature, knowledge of its risk factors, and whether it can be predicted, remains limited. This study, conducted in Norway, uses individual-level register data from 214,667 SARS-CoV-2 infected individuals covering a range of demographic, socioeconomic factors, as well as cause-specific healthcare utilization in the years prior to infection to assess the risk of post-COVID complaints ≥3 months after testing positive. We find that the risk of post-COVID was higher among individuals who prior to infection had been diagnosed with psychological (OR = 2.12, 95% CI 1.84–2.44), respiratory (OR = 2.03, 95% CI 1.78–2.32), or general and unspecified health problems (OR = 1.78, 95% CI 1.52–2.09). To assess the predictability of post-COVID after mild initial disease, we use machine learning methods and find that pre-infection characteristics, combined with information on the SARS-CoV-2 virus type and vaccine status, to a considerable extent (AUC = 0.79, 95% CI 0.75–0.81) could predict the occurrence of post-COVID complaints in our sample. In this study, the authors investigate the incidence and risk factors for post-COVID condition among people who had a mild initial SARS-CoV-2 infection in Norway. They use national linked registry data including ~215,000 individuals with a positive SARS-CoV-2 test who were not hospitalised and followed them up for 180 days after infection.
|
|
Scooped by
HAS-veille
September 19, 2023 4:08 AM
|
Description: Evidence for the use of outpatient treatments in adults with confirmed COVID-19 continues to evolve with new data. This is version 2 of the American College of Physicians (ACP) living, rapid practice points focusing on 22 outpatient treatments for COVID-19, specifically addressing the dominant SARS-CoV-2 Omicron variant. Methods: The Population Health and Medical Science Committee (formerly the Scientific Medical Policy Committee) developed this version of the living, rapid practice points on the basis of a living, rapid review done by the ACP Center for Evidence Reviews at Cochrane Austria at the University for Continuing Education Krems (Danube University Krems). This topic will be maintained as living and rapid by continually monitoring and assessing the impact of new evidence. Practice Point 1: Consider molnupiravir to treat symptomatic patients with confirmed mild to moderate COVID-19 in the outpatient setting who are within 5 days of the onset of symptoms and at a high risk for progressing to severe disease. Practice Point 2: Consider nirmatrelvir–ritonavir combination therapy to treat symptomatic patients with confirmed mild to moderate COVID-19 in the outpatient setting who are within 5 days of the onset of symptoms and at a high risk for progressing to severe disease. Practice Point 3: Do not use ivermectin to treat patients with confirmed mild to moderate COVID-19 in the outpatient setting. Practice Point 4: Do not use sotrovimab to treat patients with confirmed mild to moderate COVID-19 in the outpatient setting.
|
|
Scooped by
HAS-veille
September 6, 2023 10:14 AM
|
Preexisting medical and socioeconomic factors, as well as acute COVID-19 symptoms,
are associated with the development of and recovery from the PCC. Recovery is extremely
rare during the first 2 years, posing a major challenge to healthcare systems.
|
|
Scooped by
HAS-veille
September 5, 2023 2:38 AM
|
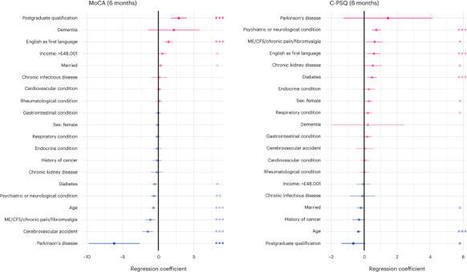
Post-COVID cognitive deficits, including ‘brain fog’, are clinically complex, with both objective and subjective components. They are common and debilitating, and can affect the ability to work, yet their biological underpinnings remain unknown. In this prospective cohort study of 1,837 adults hospitalized with COVID-19, we identified two distinct biomarker profiles measured during the acute admission, which predict cognitive outcomes 6 and 12 months after COVID-19. A first profile links elevated fibrinogen relative to C-reactive protein with both objective and subjective cognitive deficits. A second profile links elevated D-dimer relative to C-reactive protein with subjective cognitive deficits and occupational impact. This second profile was mediated by fatigue and shortness of breath. Neither profile was significantly mediated by depression or anxiety. Results were robust across secondary analyses. They were replicated, and their specificity to COVID-19 tested, in a large-scale electronic health records dataset. These findings provide insights into the heterogeneous biology of post-COVID cognitive deficits. Longitudinal proteomic profiling of over 1,800 patients revealed two distinct profiles of blood biomarkers measured on admission to hospital for COVID-19, which predict cognitive deficits 6 and 12 months later.
|
|
Scooped by
HAS-veille
August 31, 2023 7:18 AM
|
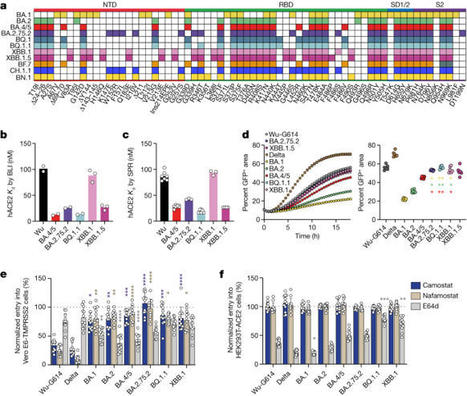
Currently circulating SARS-CoV-2 variants have acquired convergent mutations at hot spots in the receptor-binding domain1 (RBD) of the spike protein. The effects of these mutations on viral infection and transmission and the efficacy of vaccines and therapies remains poorly understood. Here we demonstrate that recently emerged BQ.1.1 and XBB.1.5 variants bind host ACE2 with high affinity and promote membrane fusion more efficiently than earlier Omicron variants. Structures of the BQ.1.1, XBB.1 and BN.1 RBDs bound to the fragment antigen-binding region of the S309 antibody (the parent antibody for sotrovimab) and human ACE2 explain the preservation of antibody binding through conformational selection, altered ACE2 recognition and immune evasion. We show that sotrovimab binds avidly to all Omicron variants, promotes Fc-dependent effector functions and protects mice challenged with BQ.1.1 and hamsters challenged with XBB.1.5. Vaccine-elicited human plasma antibodies cross-react with and trigger effector functions against current Omicron variants, despite a reduced neutralizing activity, suggesting a mechanism of protection against disease, exemplified by S309. Cross-reactive RBD-directed human memory B cells remained dominant even after two exposures to Omicron spikes, underscoring the role of persistent immune imprinting. Convergent mutations in hot spots of the spike proteins of currently circulating SARS-CoV-2 Omicron variants increase the binding affinity for the host receptor and promote more efficient fusion with host cell membranes.
|
|
Scooped by
HAS-veille
August 31, 2023 4:11 AM
|
Rigorous evidence shows that significant contact with a person with SARS-CoV-2 is more likely to lead to transmission than a short encounter.
|
|
Scooped by
HAS-veille
August 29, 2023 7:16 AM
|
Conspiracy theories comprise a dominant entity of the COVID-19 information environment and their endorsement is negatively associated with COVID-19 pr…
|
|
Scooped by
HAS-veille
August 28, 2023 2:45 AM
|
This hyper-mutated variant has shown up in many places now, at a time when wastewater and genomic surveillance is greatly diminished around the world. To date, the BA.2.86 variant has been detected in Israel, Denmark (3 individuals), the UK, the US (2 individuals, one coming back from Japan), and South Africa (2 individuals). It has also been detected in wastewater in 1 region in Switzerland (2% level), along with wastewater detection in Ohio and in Thailand. It’s safe say that BA.2.86’s presence is widespread across the world at this point.
|
|
Scooped by
HAS-veille
August 23, 2023 10:08 AM
|
Cet avis scientifique du Comité sur l’immunisation du Québec (CIQ) vise à émettre des recommandations sur la vaccination contre la COVID-19 à l’automne 2023. Les données récentes indiquent que le fardeau de la COVID-19 est concentré chez les personnes de 60 ans et plus et chez celles vivant avec certaines maladies chroniques.
|
|
Scooped by
HAS-veille
August 22, 2023 3:48 AM
|
New reports at two years and the known unknowns that lie ahead
|
|
Scooped by
HAS-veille
August 21, 2023 5:00 AM
|
|
|
Scooped by
HAS-veille
August 9, 2023 7:10 AM
|
|