Your new post is loading...
Your new post is loading...

|
Rescooped by
Gilbert C FAURE
from Immunology and Biotherapies
January 30, 2020 1:15 PM
|
Point of view of an Immunologist/curator in 2020 Après Bobcatsss 2020, ECIL 2021, ICDF 2022, HESIVAXs with the motto UTA "Understand to Act" Notre proposition « Désinformation Vaccinale: Curation, Observatoire, Littératies » a été retenue pour le séminaire annuel de l’Académie des Controverses et de la Communication Sensible, intitulé « La désinformation : nouvelles formes, nouveaux défis », qui s'est tenu à Paris le mardi 26 novembre 2024. Voir ci-après posts du 27 novembre, avec lien vers la présentation sur Slideshare. Présentation le 20 mars 2025 à InfoxsurSeine deux jours pour décrypter la désinformation et échanger autour des solutions.
Quels outils concrets face aux manipulations de l’information et à l’essor de l’IA générative ? Avez vous acheté le numéro Juillet/septembre 2025 de la RECHERCHE sur LE FAUX? des sujets à approfondir - Vaccins et argent Making money with vaccines, against vaccines le sujet le plus chaud, de 3,36 euros par mois à 300 millions de dollars? - Publications vraies et fausses particulièrement difficile - Obligations, exemptions, incitations, peut-être plus simple?
|
|
Scooped by
Gilbert C FAURE
Today, 4:10 AM
|
Interest in ‘toxic’ measles treatment surges after Joe Rogan podcasts
“Vaccination is the only proven way to prevent measles - but alternative treatments such as Vitamin A and cod-liver oil (which contains large quantities of Vitamin A) have been promoted in the media by public figures such as Joe Rogan,” the authors of a new research paper said in JAMA Network said.
“Medical professionals may give measles patients Vitamin A to help support their recovery, but it doesn’t prevent measles and can be toxic in large doses.”
The researchers examined online search trends and found that statements in the media declaring Vitamin A a measles treatment were associated with a surge in related web searches.
While focusing on government statements, the researchers said they also factored in statements by figures such as Rogan and vaccine sceptic Dr Suzanne Humphries.
At about the same time, America’s Poison Centres reported a 39 per cent increase in Vitamin A exposures.
Source in comments.
|
|
Scooped by
Gilbert C FAURE
Today, 4:05 AM
|
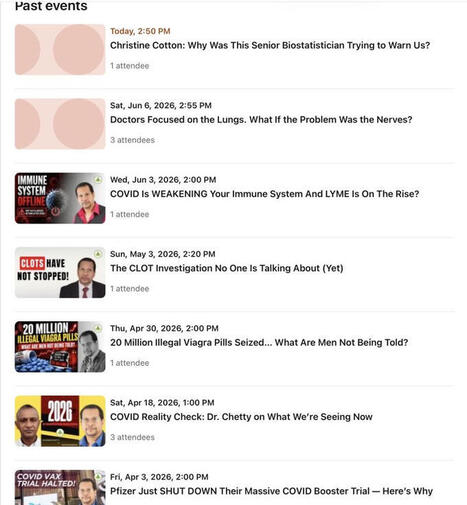
Is there an appetite for scientific conspiracy theories ?
Is there one for pseudoscientific pseudodoctors on this platform ?
Well, let’s look at the number of participants at these events only to realize that there is none. And why lose his time doing such as no one attends ? Is his time so not precious that 1-3 attendees per event would acceptable return on investment ?
|
|
Scooped by
Gilbert C FAURE
Today, 4:01 AM
|
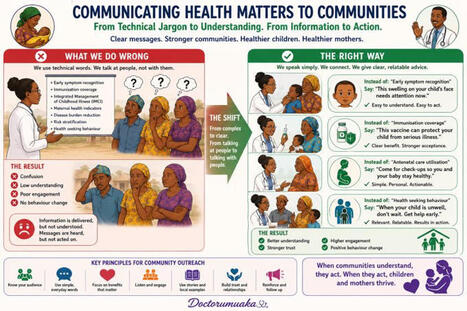
The day a conversation about children changed the way I think about public health communication.
I recently participated in a discussion on communicating with children. A presenter said 'communicate in an age appropriate manner'
Another presenter made a simple but profound statement:
"Speak the language they understand,
not just the language they hear."
The language they understand.
It got me thinking about how often we approach communities the same way we sometimes approach children: with information that makes sense to us, but not necessarily to them.
As health professionals, advocates, researchers, and policymakers, we spend years learning technical terms. We become fluent in statistics, guidelines, protocols, and evidence.
Then we walk into a community with beautifully planned outreaches, blow a lot of grammar and go home.
We come back to access impact of what we came to preach about, and wonder why behaviour doesn't change.
The truth is that behavioural change rarely happens because people received information. It happens because people received information they could connect with.
A mother in a rural community may not understand "early symptom recognition," but she understands:
"This swelling on your child's face is not something to watch for six months."
A father may not understand "immunisation coverage," but he understands:
"This vaccine can help protect your child from getting seriously ill, reduce hospital admissions and save the family money."
A community leader may not understand "cancer prevention strategies," but he understands:
"If we find this disease early, more of our people will most likely survive it"
The gap between what experts say and what communities hear is often where good programmes go to die.
Whether we are discussing malaria, maternal health, immunisation, nutrition, or cancer, our success depends not on how much we know, but on how well we translate what we know into words that matter to the people we serve.
And perhaps nowhere is this more important than when we talk about children.
Children cannot advocate for themselves.
For many childhood illnesses, including cancers, the adults around them are the ones who must notice the signs, seek help, and act early.
If our messages are not understood, opportunities for early diagnosis and prompt treatment are probably lost.
Maybe the next frontier in public health is not producing more information.
Maybe it is becoming better translators of information.
Because communities do not change when we speak.
Communities change when they understand.
#Healthcommunication #CommunityHealth #ChildHealth #Paediatrics #Doctorumuaka
|
|
Scooped by
Gilbert C FAURE
Today, 4:00 AM
|
Del Bigtree goes on tour and likely neglects to mention that countries like Poland and France, with similar immunization schedules to the United States, have much lower rates of autism. https://lnkd.in/gGYeATxn
|
|
Scooped by
Gilbert C FAURE
Today, 3:57 AM
|
Did you know that up to 95% of polio infections are asymptomatic?
Polio is a viral infection that often causes no noticeable symptoms. When symptoms do occur, they may include a low-grade fever and sore throat. In some cases, symptoms can progress after a few days to include stiffness of the neck, back, or legs.
For those interested in learning more, we've included a resource in the first comment.
#vaccines
|
|
Scooped by
Gilbert C FAURE
Today, 3:49 AM
|
|
|
Scooped by
Gilbert C FAURE
June 7, 11:43 AM
|
This Is How Low Anti-Vaccine Influencers Will Go
|
|
Scooped by
Gilbert C FAURE
June 7, 3:55 AM
|
Article 537534 publicat a IMC BCN de forma directa, autogestionada i segura. Articulo 537534 publicado en IMC BCN de forma directa, autogestionada y segura.
|
|
Scooped by
Gilbert C FAURE
June 7, 3:54 AM
|
Unjected and PureBlood.Dating are hosting in-person meetups—and have transformed the dating landscape into a political battleground over bodily autonomy.
|
|
Scooped by
Gilbert C FAURE
June 7, 3:38 AM
|
Les recommandations vaccinales sont aujourd’hui largement établies. Pourtant, leur diffusion reste un défi.
Le Dr Pierre Loulergue, spécialiste des maladies infectieuses à l’AP-HP, Assistance Publique - Hôpitaux de Paris, revient sur les enjeux actuels de la vaccination en France : mieux informer, mieux accompagner et faciliter l’accès à la prévention à chaque étape de la vie.
Pourquoi certaines recommandations restent-elles encore mal connues ? Comment renforcer le rôle des soignants dans la pédagogie vaccinale ? Quels leviers pour améliorer durablement la couverture des Français ?
Pour assister à cette table ronde 👇
📍 En visio-conférence
📅 Jeudi 21 mai 2026 | 16h30 – 17h00
🔗 Programme complet et inscriptions : https://lnkd.in/dGz-xuir
Un événement Villa M, en partenariat avec Le Point
#DialoguesDeLaSanté #vaccination #santépublique #prévention #VillaM
|
|
Scooped by
Gilbert C FAURE
June 7, 3:35 AM
|
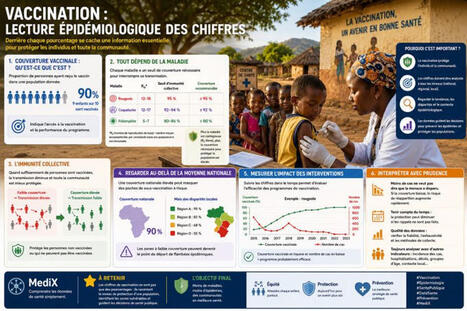
𝐕𝐚𝐜𝐜𝐢𝐧𝐚𝐭𝐢𝐨𝐧 : 𝐥𝐞𝐜𝐭𝐮𝐫𝐞 𝐞́𝐩𝐢𝐝𝐞́𝐦𝐢𝐨𝐥𝐨𝐠𝐢𝐪𝐮𝐞 𝐝𝐞𝐬 𝐜𝐡𝐢𝐟𝐟𝐫𝐞𝐬
La vaccination est souvent résumée à un simple pourcentage : 50 %, 70 % ou 90 % de couverture vaccinale. Pourtant, en épidémiologie, ces chiffres ont une signification bien plus profonde. Bien les interpréter permet de comprendre l’efficacité des programmes de vaccination et leur impact sur la santé publique.
Le premier indicateur que l’on observe est la #couverture_vaccinale. Elle représente la proportion de personnes ayant reçu un vaccin dans une population donnée. Par exemple, si 9 enfants sur 10 sont vaccinés contre la rougeole, la couverture vaccinale est de 90 %. Cet indicateur permet d’évaluer l’accès à la vaccination et la performance des programmes de santé.
Cependant, une couverture élevée ne garantit pas toujours une protection suffisante. Tout dépend de la maladie concernée. Certaines infections très contagieuses, comme la rougeole, nécessitent une couverture vaccinale supérieure à 95 % pour limiter efficacement la circulation du virus. À l’inverse, d’autres maladies peuvent être contrôlées avec des niveaux de couverture plus faibles.
L’un des concepts les plus importants est celui de #l_immunité_collective. Lorsqu’une proportion suffisamment importante de la population est vaccinée, la transmission de la maladie diminue fortement. Les personnes non vaccinées ou celles qui ne peuvent pas être vaccinées bénéficient alors d’une protection indirecte. La vaccination protège donc non seulement l’individu, mais également la communauté.
L’analyse des chiffres permet aussi de détecter des zones à risque. Une couverture vaccinale nationale de 90 % peut sembler satisfaisante, mais si certaines régions affichent seulement 60 % ou 70 %, des flambées épidémiques peuvent toujours survenir. C’est pourquoi les épidémiologistes analysent les données à différentes échelles : nationale, régionale et locale.
Un exemple concret est celui de la rougeole.
Plusieurs pays ont connu des résurgences de la maladie malgré une couverture vaccinale nationale relativement élevée. Les analyses ont montré que certains groupes ou territoires présentaient une couverture insuffisante, créant des poches de population vulnérable où le virus pouvait continuer à circuler.
Les chiffres de la vaccination permettent également de mesurer l’impact des interventions de santé publique. Une augmentation progressive de la couverture vaccinale, associée à une diminution du nombre de cas, constitue souvent un indicateur fort de l’efficacité d’un programme de vaccination.
Cependant, ces données doivent être interprétées avec prudence.
Une baisse du nombre de cas ne signifie pas toujours que la menace a disparu. Si la couverture vaccinale diminue avec le temps, le risque de réapparition de la maladie peut augmenter rapidement.
#Epidemiologie #Vaccination
#SantéPublique #DataSanté #Biostatistique #Prévention #MediX
|
|
Scooped by
Gilbert C FAURE
June 7, 3:10 AM
|
A few years ago, I believed that improving health was mostly about medicine, diagnoses, and access to healthcare.
After working in public health across different communities, I realized something much bigger:
Many of the factors that shape a person's health have very little to do with what happens inside a clinic.
I've met families who wanted healthier lives but struggled with housing insecurity. I've seen students whose academic performance was affected by food access. I've worked with communities where transportation, language barriers, or limited resources made even basic healthcare difficult to reach.
Health is influenced by where we live, learn, work, and grow.
That's why some of the most meaningful public health work doesn't happen in a laboratory or hospital. It happens in neighborhoods, schools, community centers, and through conversations that help people feel seen, supported, and connected.
One lesson I've carried throughout my career is this:
If we want healthier communities, we must invest in people before they become patients.
Every small effort matters. Every mentor matters. Every teacher, volunteer, healthcare worker, community leader, and advocate matters.
Creating healthier communities is not the responsibility of one profession. It's something we build together.
What is one non-medical factor that you believe has the greatest impact on a person's health and well-being?
#PublicHealth #CommunityHealth #HealthEquity #PopulationHealth #Healthcare #MentalHealth #PublicHealthLeadership #SocialDeterminantsOfHealth #CommunityImpact #Leadership
|
|
|
Scooped by
Gilbert C FAURE
Today, 4:19 AM
|
|
|
Scooped by
Gilbert C FAURE
Today, 4:06 AM
|
The Fastest Way to a Million Views? Become a Healthcare Influencer.
In today's digital landscape, credentials and years of training seem to take a backseat to sensationalism. The journey of a doctor, with its sleepless nights and significant debt, is overshadowed by the allure of viral content by non doctors- because none of that matters when a guy with a Ring Light and a podcast microphone has already cracked the code. Want views? It’s simple. Do a podcast on healthcare for starters!!! Start with a provocative statement like "doctors are lying to you" "Hospitals are looting you" and watch the algorithm bless you like a long-lost child.
The formula is straightforward:
- Begin with "the healthcare system is broken" — a true statement, but not the reason for your message.
- Quickly pivot to insinuating that physicians are on pharmaceutical payrolls, without citing any evidence. Citations slow down the momentum.
- Hospital bills? Magnificent content. Pick a $90,000 invoice, zoom in dramatically, and ask with wide eyes "why does a Band-Aid cost $47?" Don't mention the uncompensated care, the malpractice insurance, the regulatory compliance, the 24/7 staffing model, or the fact that nobody actually pays that number — that would be journalism, and journalism doesn't trend.
The narrative continues - try another bait, exodus of doctors to foreign land after taking subsidized medical education in home country. Frame it as a betrayal of national resource, ignoring the complexities of burnout and systemic issues. Instead, rely on anecdotal evidence from social media comments.
Ironically, the same author / audience that shares these critical views when sick will find themselves in an ER, grateful for the trained professionals who show up, ready to help despite the challenges. So, go ahead and drop that episode. The views will be excellent.
*(Thank you to all the non-doctors ranting about medicine on social media. While you're busy collecting views, likes, and podcast subscribers, the people who actually understand healthcare are busy collecting night shifts, difficult decisions, and lives saved).
|
|
Scooped by
Gilbert C FAURE
Today, 4:02 AM
|
It does not seem like measles is “under control” as of today, June 6, 2026. CDC’s latest update, posted June 5 and reflecting data through June 4, reports 2,030 confirmed measles cases in 2026, across 40 jurisdictions, with 30 new outbreaks this year and 93% of cases outbreak-associated. That is not a contained, isolated situation. It means transmission is still occurring in clusters, mostly among under-vaccinated communities. The core public-health problem is that measles control depends on extremely high vaccination coverage because measles is one of the most contagious human viruses. CDC states that when more than 95% of people in a community are vaccinated, most people are protected through community, or herd, immunity; the warning sign is that U.S. kindergarten MMR coverage has fallen below that level, dropping from 95.2% in 2019–2020 to 92.5% in 2024–2025 and leaving roughly 286,000 kindergartners without documented completion of the MMR series (Centers for Disease Control and Prevention [CDC], 2025, 2026). That gap matters because national averages can hide vulnerable local pockets, and CDC explicitly warns that when measles enters communities with lower vaccination rates, outbreaks can occur and spread quickly (CDC, 2026). So no, measles is not “under control” in the meaningful public-health sense: it is vaccine-preventable, but the protection wall has thinned below the herd-immunity threshold, which means the virus has more openings to move through under-vaccinated communities.
|
|
Scooped by
Gilbert C FAURE
Today, 4:01 AM
|
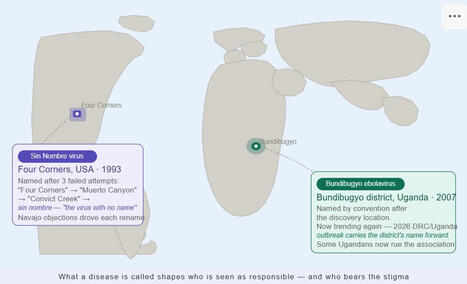
Two viruses. Two naming decisions. One lesson for public health communicators.
When the 1993 Four Corners hantavirus outbreak was identified, scientists followed convention and proposed naming the new pathogen after its location — first "Four Corners virus," then "Muerto Canyon virus" after a site on the Navajo Reservation.
The Navajo Nation objected to both. The outbreak had already caused serious harm: events were relocated, and Navajo people were refused service at businesses and required to undergo medical testing to visit college campuses. Scientists tried "Convict Creek virus." Rejected too. Tribal elders appealed directly to officials, and the pathogen was finally named Sin Nombre — "the virus with no name."
Contrast that with Bundibugyo. Named after a mountainous district in western Uganda following a 2007 outbreak, the district is now trending again — the current Ebola outbreak in DRC and Uganda has made some Ugandans rue the association with a disease carrying a 30–50% case fatality rate.
The two cases represent opposite failure modes in disease naming. Sin Nombre shows what happens when a community already stigmatized by an outbreak has a geographic name compound the harm. Bundibugyo shows that even a "neutral" name, applied without stigma at the time, can become a burden decades later when it resurfaces in a new outbreak.
Three things this means for behavioral scientists and health communicators:
Names are frames. What a disease is called shapes who is seen as at risk, who is blamed, and who deserves sympathy. Your messaging strategy inherits whatever the name communicates.
Community resistance is data, not obstruction. The Navajo Nation's objections were a signal that scientists were underestimating social consequences. That signal produced a better outcome. When communities push back on how a health problem is labeled, treat it as information.
The window for getting it right is narrow. By the time scientists proposed "Muerto Canyon" in January 1994, early media framing had already done its damage. Naming — and the community engagement that should precede it — needs to happen at the start of a response, not after the headlines have written the story.
Sin Nombre got its name because a community pushed back hard enough, and scientists listened. That's a model worth remembering.
#BehavioralScience #HealthCommunication #VaccineConfidence #PublicHealth #Hantavirus #Ebola #Bundibugyo #RiskCommunication #HealthEquity #Stigma #Infodemic #GlobalHealth #ABSN #BiL
|
|
Scooped by
Gilbert C FAURE
Today, 3:58 AM
|
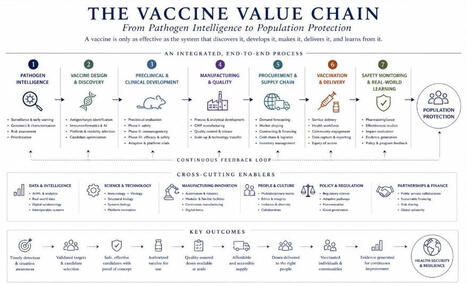
One lesson repeatedly emerges from the history of vaccinology.
When an outbreak occurs, attention naturally focuses on the vaccine itself. Do we have one? How effective is it? How quickly can it be deployed?
These are important questions, but they are incomplete.
A vaccine is only one component of a much larger system. Before a vaccine can protect a population, pathogens must be detected, characterized, and understood. Candidates must be designed and evaluated. Manufacturing processes must be developed and validated. Regulatory pathways must function. Supply chains must deliver potent product to the point of care. Safety and effectiveness must continue to be monitored long after deployment.
Failures rarely occur within a single discipline. More often, they occur at the interfaces between disciplines.
The attached figure is an attempt to represent vaccinology as an ecosystem rather than a sequence of isolated activities.
The history of vaccines teaches us that scientific discovery is indispensable. It also teaches us that discovery alone is never sufficient.
The value of a vaccine is ultimately determined by the strength of the system that surrounds it.
As data science, artificial intelligence, and platform technologies become increasingly integrated into vaccine development, understanding these interfaces may become even more important than understanding any individual component.
|
|
Scooped by
Gilbert C FAURE
Today, 3:51 AM
|
La vidéo d’une journaliste scientifique autrichienne complotiste a refait surface sur X.Dans ces images datant de 2009, elle y accuse l’OMS d’orchestrer un complot mondial pour prendre le contrôle de la population...
|
|
Scooped by
Gilbert C FAURE
June 7, 11:45 AM
|
This week, we attended the 2026 Kansas Immunization Conference, where immunization champions from across the state came together to connect, collaborate, and share ideas. It was a great opportunity to showcase our immunization resources and materials, including our new HepB campaign in partnership with The Kansas Chapter, American Academy of Pediatrics (KAAP), and the Kansas Hospital Association.
We also had the opportunity to learn from many notable speakers, including Karen Ernst, Director of our national partners, Voices for Vaccines, who shared insights on becoming a trusted messenger. Dr. Gretchen Homan, a long-standing IKC member and pediatrician, along with Dr. Eddie Lyon, pediatrician and IKC Board member, also shared valuable perspectives as providers navigating immunizations and communicating their importance to patients.
A big thank you to the Kansas Department of Health and Environment's Kansas Immunization Program for hosting such an impactful conference! 🌻 🌟 🩹
➡️ View our new campaign resources: https://lnkd.in/gCva5VST
|
|
Scooped by
Gilbert C FAURE
June 7, 11:41 AM
|
77 Cases and Climbing — Virginia Is Facing Its Worst Measles Outbreak in Years.
Virginia health officials are sounding the alarm as measles infections continue spreading across the state in what they are calling a crisis "unlike anything we've seen in years."
The Virginia Department of Health is now reporting at least 77 confirmed cases, with most infections linked to ongoing transmission in Central Virginia. Health teams are watching the numbers rise in real time — and they say the outbreak is moving fastest through communities where vaccination coverage is lowest, creating dangerous immunity gaps that are making containment harder with every passing day.
Contact tracing is underway and public health teams are actively monitoring every new case as they work to prevent fresh clusters from forming. Officials are urging every resident — especially in high-exposure areas — to check their vaccination status and get fully vaccinated if there is any doubt.
Measles was declared eliminated in the United States in the year 2000. What is happening in Virginia right now is a warning about what comes when vaccination rates fall.
|
|
Scooped by
Gilbert C FAURE
June 7, 3:54 AM
|
IMC committee found De Brun guilty of professional miscondcut...
|
|
Scooped by
Gilbert C FAURE
June 7, 3:39 AM
|
In what may be a new low for anti-vaccine influencers, Lara Logan pushes the idea that kids in South Sudan would be better off without vaccines. https://lnkd.in/gm6Un-NY
|
|
Scooped by
Gilbert C FAURE
June 7, 3:35 AM
|
A polio survivor became a leading voice helping other children get vaccinated and protected!
"I contracted polio as a toddler. It is a very contagious virus that attacks an infected person’s brain and can lead to paralysis.This was the future my parents set in motion when they opted not to have me vaccinated."
https://lnkd.in/gsS-2yRs
|
|
Scooped by
Gilbert C FAURE
June 7, 3:11 AM
|
News about our next Citizen Science for Health conference 👇
This edition’s conference theme is: “The Societal Impact of Citizen Science for Health”. And we are now inviting submissions for conference abstracts.
⭐ The conference aims to introduce state-of-the-art in the CS4H domain and continue the transition from long-standing traditions of patient participation in health research to more recent and intensive modes of citizen science in health.
💪 Impact can be defined as the effects of research and innovation beyond academia, including effects on society, the economy, the environment, and policy. In connection, the conference has special focuses on women’s health, health inequality, trans- and interdisciplinary research approaches, ethics and the sharing and co-production of data.
🤝 We invite citizen perspectives as well as contributions regarding emerging work from young career researchers. Both theoretical and empirical perspectives on these themes are invited.
⏰ Abstract submission deadline: 1 September 2026, 23:59 CEST
🔗 Submit your abstract here: https://lnkd.in/eSx-rMWs
|
|
Scooped by
Gilbert C FAURE
June 7, 3:08 AM
|
This headline caught my attention this morning. (Particularly because Gather Voices will be working with the American Public Health Association next week in DC.)
“Hospitals See Diseases Resurge as Vaccinations Decline.”
Whether you’re talking about vaccines, public policy, media, science, business, or associations, there’s a bigger story underneath it:
Trust in institutions is declining.
People are increasingly skeptical of experts, authorities, governments, media outlets, and organizations of every kind.
The frustrating part is that many of the things that make society work depend on a baseline level of trust. Public health is one example. Professional standards, continuing education, advocacy, and even events are others.
When trust erodes, it becomes harder to get people to take actions that are objectively in their own interest.
But complaining about that reality doesn’t change it.
Organizations have to operate in the world as it exists, not the one we wish existed.
The good news is that while trust in institutions may be declining, trust in peers remains remarkably resilient.
People still listen to:
• People like themselves
• People they know
• People who share their experiences
• People they perceive as authentic
That has implications for every organization trying to educate, persuade, recruit, advocate, or inspire action.
Instead of relying exclusively on expert-to-audience communication, we need to think more about enabling peer-to-peer communication.
Not replacing expertise.
Amplifying it through trusted voices.
The organizations that figure out how to combine expertise with authentic stories from real people will have a significant advantage in the years ahead.
Trust may be harder to earn than it used to be.
But it can still be earned.
Often one real voice at a time.
|