Virtual reality, with the requisite head gear, can make you a more caring, helpful person, Stanford University researchers say. The WSJs Michael Kofsky steps into computer-generated worlds to test their claims.
Dr Nikki Goldstein, Sexologist and Relationship expert said “When it comes to sex, people often focus the majority of importance on penetration rather than touch, which can be vital for intimacy, sexual pleasure and relationship satisfaction. When we touch someone we have the ability to connect with them, allow them to feel secure and desired, and even release sex hormones that can help us get in the mood.
Virtual Occupational Therapy Assistant was developed in recognition of the need for a gaming application for stroke therapy that is fun, accessible, and meaningful in the context of occupational therapy objectives -- in other words relearning skills that permit functional independence at home.
When placed in a virtual environment with three hills of different heights and angles of incline, participants who customized their avatars perceived those hills as higher and steeper than participants who were assigned avatars by the researchers, Sundar says. They also overestimated the amount of calories it would take to hike up the hill if their custom avatar had a backpack.
Welcome to the Games and Simulation for Healthcare Library and Database. This website aims to provide a portal and network to meet the needs of clinicians, researchers and educators in the healthcare community who want to integrate games and simulation into their scholarship and patient care strategy. This resource also welcomes healthcare consumers, advocates, and others interested in patient and clinician education, and clinical research taking advantage of games and simulation-based learning.
Please visit frequently and feel free to contact our project team for details on how you can contribute to this project, or with any comments and suggestions.
1. The integration must take into account each user’s day-to-day life and workflow, including patients, providers, IT staff, and additional caregivers. Some users will need access to a greater depth of information, while for others design and usability will be paramount.
2. The design should be interoperable and support the integration of multiple MITs into a single EHR. In particular, developers should make sure to eliminate redundancies between the systems, where app users and EHR users might enter the same data into different fields.
3. Multiple environments have to be secure, but their security can’t keep them from interacting with each other. Stakeholders WellDoc interviewed reported problems with competing firewalls in implementing the integration.
4. Both halves of the integration, but especially the patient-facing app, should work natively on as many mobile devices as possible. Patients are most likely to use a system that allows them to continue using their device.
5. The mobile health offering is subject to a limitation already standard for EHR apps: it must be able to run even when network connectivity is sparse or intermittent, as is sometimes the case in large hospital complexes.
6. It’s crucial to have a support team in place familiar with the technology to help acquaint users with it.
7. Make sure the two systems adhere to common standards. Not only data interchange standards like HL7, but also making sure that measurements in both systems use the same units. If lab-collected blood glucose data in the EHR and patient-collected blood glucose data have the same unit, but one is potentially more accurate, the integrated system should easily identify and distinguish the two.
8. The team working on an integration should be ready for a more complex process than anticipated. A clear vision, good communication, and a steering committee are important for anyone attempting to integrate a mobile heath offering and an EHR.
Health Apps allowing more transparancey and awareness in the health sector. This means that patients can become proactive in their treatment process. #patientchampions
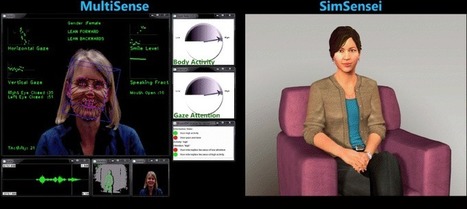
Temple researchers are developing a virtual speech therapist that could someday help people like Green by providing a more accessible and cost-effective tool for the repetition and practice exercises that are crucial to recovery.
The two-year study, which is being conducted by Temple’s Nadine Martin, professor of communication sciences; Emily Keshner, professor and chair of physical therapy; and Justin Shi, associate professor of computer science; along with Alex Rudnicky, professor of computer science at Carnegie Mellon University, is supported by a new $275,000 R21 NIH grant.
Mayor Jim Ardis said it would be a recruiting tool for the world’s leading researchers and doctors.
Speakers, from Robert Easter, president of the University of Illinois system, to Sister Judith Ann Duvall, chairwoman of the OSF Healthcare System board, paid tribute to Bill DiSomma, a managing partner in the Chicago-based trading firm, Jump Trading, whose $25 million donation made the center possible.
Some more great work from Virtual Ability, Inc, with this Saturday seeing a Mental Health Symposium. You can find out more on the Virtual Ability blog but here's the schedule: Will you Treat ME? F...
There are other advantages. Researchers can build an entire bar to simulate a drinking environment (and, in fact, they have), but it's more economical to use a virtual environment, where fake components get plopped into place - no moving parts necessary.
Until we find out exactly how effective virtual reality cue reactivity is for treating substance abuse, Rosenthal is supplementing his research with more traditional (but still novel) methods. Subjects in his virtual environment are played electronic blips after they start to come down, and later, when they get cravings in the real world, they can call a number to hear the tones again, assuaging the craving. That's a parallel for how virtual reality cue reactivity will likely be used: as a secondary world, not a replacement for the real one.
In the film, Iron Man 3, the good guys encase themselves in tech. The bad guys put the tech inside their bodies. This is telling. Hollywood - and most of
A free resource that uses interactive video and games-based learning to teach students vocabulary. Educators can set school tournaments, and students can play fun learning games challenging classmates and other schools.
"A group of Harvard education researchers have developed a virtual simulation for “walking in another person’s shoes” to help students relate to one another better. It’s part of a project calledSocial Aspects of Immersive Learning (SAIL) funded by the National Science Foundation. “The ability to accurately read people is really important to make compromises,” said Elisabeth Hahn, a doctoral candidate at the Harvard School of Education in a recent edWeb webinar"
The ability to place students in a safe simulation to experience how someone else has to live, I have found to be a powerful learning experience for college students who will be dealing with challenged children in the future classrooms.
This course examines the implications of informatics for practice, in nursing, public health, and healthcare in general. It covers electronic health record issues and relates ethical, legislative and political issues to health informatics. Students will also explore global and future informatics issues.
For decades the goal of tissue engineers has been to advance beyond two dimensional cell cultures to create three dimensional organs. While growing organs (e.g. human bladders) from scratch on scaffolds has already been achieved, there was no highly accurate method to build three-dimensional cellular and/or polymeric structures. Existing technology lacked architectural integrity, had degradation problems with scaffold usage, was prone to subjective human interaction, and lacked automated, scalable processes capable of creating therapeutic tissues for commercial applications in clinical settings.
Mobile health applications represent the next stage of patient empowerment. 30 years ago, patients received information and procedures from their physicians, often without instruction. Now, the smartphone physical empowers patients to identify, understand, and manage their own health on a completely new level. This offers critical implications for the future of medicine:
1. Patient Engagement: It’s probable that the physical act of regularly checking blood pressure or measuring blood sugar levels can make a patient more conscious about their health. It’s also hopeful that such self-tracking can inspire self-education and positive behavior change. This is difficult to measure experimentally (have you ever noticed that the most avid quantified self-ers are the fittest and healthiest people?) but it offers reason to be optimistic about mHealth.
2. Remote Care: A critical challenge of hospital readmissions is that, once the patient walks out the door, it’s no easy endeavor to reconnect with them. If physicians could remotely monitor patients, it’s possible they could identify early signs of a complication and intervene. As a readmissions researcher, I’ve spoken with patients who waited for three weeks of not being able to eat before returning to the hospital 30 pounds lighter. The smartphone physical could have flagged that—and someday, it will.
3. The Doctor’s Role: This is the big question, and it’s a loaded one. How will physicians interpret and process the information overload that follows such complete self-quantification? How will electronic health records and/or personal health records adapt to meaningfully consolidate, analyze, and present all this data? How does the patient’s ability to self-educate, self-diagnose, and (perhaps eventually) self-treat change the purpose and significance of the doctor-patient relationship? At Millennial Medicine, Dr. Eric Topol presented these mHealth innovations and said, “With this, why would you want to go to the hospital?” Good question — Will patients still want, or need, to interact with their doctors?
These are ambitious goals, but with the advances I’ve seen in this video as well as other seminal achievements made in mHealth and digital medicine recently, I’m optimistic that they are all entirely doable. I’m also conscious of how often I’ve used the word “possible” in this reflection and how scarcely I’ve said “proven.” It simply speaks to the fact that we’re faced with inspiring technical capabilities that offer tremendous hope; the challenge now falls to tomorrow’s physicians and scholars to innovate, research, and troubleshoot to bring these ambitions to realization.
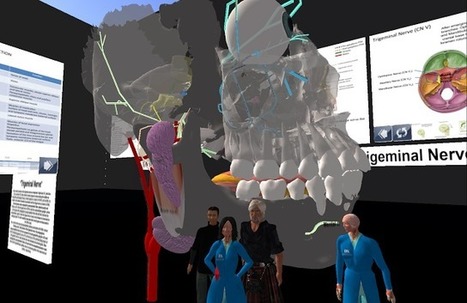
The University of Kentucky (UK) has had a strong presence in SL for some years with classes in Virtual Anatomy showing off complex parts of the human body, in particular to teach students various aspects of the cranial nervous system. They have created a “Cranial Nerve Skywalk” in Second Life that features a 3D display of cranial nerves III, V, VII, and IX. This can be seen HERE.
UWA's Professor Stuart Bunt and his student Khaleel Sunba have kicked off a collaboration with the UK's Dr April Richardson-Hatcher and Matt Hazzard with the assistance of UWA SL founder, Jay Jay Jegathesan as one of the first steps towards building a School of Anatomy, Physiology and Human Biology in Second Life. One of the triggers for the collaboration was funding from an Improving Student Learning Grant from UWA’s Centre for the Advancement of Teaching and Learning.
Journal of Interactive Learning Research ISSN 1093-023X Volume 24, Issue 3, July 2013 Association for the Advancement of Computing in Education (AACE) Chesapeake, VA
Author
Liz Falconer, University of the West of England, United Kingdom
Abstract
This paper describes and discusses a case study of postgraduate students undertaking accident investigation and risk assessment exercises in an online virtual world as part of their course curriculum. These exercises were constructed to overcome the ethical and practical barriers inherent in real-world exercises. In particular this paper focusses upon the potential of such exercises to facilitate the authentic dimension of situated learning and identifies some of the factors that affect the sense of authenticity in virtual world learning exercises. Thirteen such factors were identified. Nine of those were positive factors that enhanced the sense of authenticity; these were facilitation, presence and authority, visual realism, socialisation, comparative reality, engagement, active learning, generalizability and enabling learning from mistakes. The 4 negative factors which detracted from the sense of authenticity were the public image of virtual worlds, lack of naturalism, unrealistic graphics and lack of tactile sense.
A VIRTUAL reality teaching program by UWA and collaborators has received an international award for innovative learning using Second Life.
Now with funding from UWA’s Centre for the Advancement of Teaching and Learning, Professor Stuart Bunt from School of Anatomy, Physiology and Human Biology and student Khaleel Sunba, will explore how this 3D web-based environment can contribute to innovative changes in science teaching.
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.



 Your new post is loading...
Your new post is loading...








![11 Incredible Innovations in 3D Bioprinting [PHOTOS] | Simulation in Health Sciences Education | Scoop.it](https://img.scoop.it/BQTN34MIsY_yzXwsovheUzl72eJkfbmt4t8yenImKBVvK0kTmF0xjctABnaLJIm9)