5 juillet 2021 Une équipe de scientifiques internationaux a récemment identifié des anticorps ultrapuissants anti-coronavirus 2 (SRAS-CoV-2) anti-syndrome respiratoire aigu sévère provenant de donneurs convalescents. Les anticorps sont capables de neutraliser une large gamme de variantes du SRAS-CoV-2, même à des concentrations sous-nanomolaires. De plus, les combinaisons de ces anticorps réduisent le risque de générer des mutants d'échappement in vitro. L'étude a été publiée le 13 août 2021 dans la revue Science. https://www.science.org/doi/full/10.112 ... ce.abh1766 Sur le fond Le coronavirus 2 du syndrome respiratoire aigu sévère (SRAS-CoV-2), l'agent pathogène responsable de la maladie à coronavirus 2019 (COVID-19), est un virus à ARN simple brin enveloppé de sens positif appartenant à la famille des bêta-coronavirus humains. La glycoprotéine de pointe sur l'enveloppe virale est composée de deux sous-unités S1 et S2. Dont, la sous-unité S1 se lie directement au récepteur de l'enzyme de conversion de l'angiotensine 2 (ACE2) de la cellule hôte via le domaine de liaison au récepteur (RBD) pour initier le processus d'entrée virale. La majorité des anticorps thérapeutiques contre le SRAS-CoV-2 ont été conçus sur la base de la séquence de protéine de pointe native trouvée dans la souche Wuhan originale du SRAS-CoV-2. Ainsi, de nouvelles variantes virales avec de multiples mutations de la protéine de pointe peuvent probablement développer une résistance contre ces anticorps. Dans ce contexte, des études ont montré que les anticorps développés en réponse aux vaccins COVID-19 actuellement disponibles ont moins d'efficacité pour neutraliser les nouvelles variantes préoccupantes (COV) du SRAS-CoV, notamment B.1.1.7, B.1.351, P1 et B.1.617.2. Dans la présente étude, les scientifiques ont isolé et caractérisé des anticorps anti-pic RBD de patients guéris du COVID-19. Identification des anticorps Les anticorps ont été isolés de quatre donneurs convalescents infectés par la souche Washington-1 (WA-1) du SRAS-CoV-2. La séquence de pointe dans la souche WA-1 est similaire à la séquence de pointe dans la souche originale de Wuhan. Les cellules B isolées à partir d'échantillons de sang provenant de donneurs ont été triées pour l'identification des anticorps. Cela a conduit à l'identification de quatre anticorps neutralisants puissants ciblant le pic RBD. Ces anticorps ont montré une forte affinité pour le pic SRAS-CoV-2 même à des concentrations nanomolaires. Pour déterminer si les anticorps hautement puissants pouvaient bloquer l'ACE2 - la liaison aux pointes, des tests d'interférométrie par compétition ACE2 et de liaison à la surface cellulaire ont été effectués. Les résultats ont révélé que sur 4 anticorps, deux liés aux RBD en « position haute » et deux liés aux RBD en « position basse ». De plus, trois anticorps sur quatre bloquaient directement l'interaction RBD - ACE2, et un inhibait indirectement l'interaction par encombrement stérique - le ralentissement des réactions chimiques dû à l'encombrement stérique. Neutralisation médiée par les anticorps Tous les anticorps expérimentaux ont montré une puissance significativement plus élevée dans la neutralisation des variants contenant la mutation D614G que la souche WA-1. Une analyse plus poussée avec des particules lentivirales pseudotypées avec des variantes à pointes a indiqué que les anticorps maintiennent une puissance élevée pour neutraliser un ensemble diversifié de 10 variantes à pointes. Il est important de noter que trois des quatre anticorps expérimentaux ont montré une grande efficacité pour neutraliser 13 variantes circulantes préoccupantes/intéressantes du SRAS-CoV-2, notamment B.1.1.7, B.1.351, B.1.427, B.1.429, B.1.526, P.1, P.2, B.1.617.1 et B.1.617.2. Analyse structurale et fonctionnelle des anticorps Des analyses au microscope cryoélectronique des structures du complexe anticorps-antigène ont révélé que deux anticorps avec le pouvoir de neutralisation le plus élevé se lient à la protéine de pointe avec tous les RBD en « position haute ». D'autres analyses structurelles ont révélé que les modes de liaison à l'épitope des anticorps sont responsables d'un pouvoir neutralisant élevé contre les COV du SRAS-CoV-2. La capacité de liaison et de neutralisation des anticorps a été affectée négativement par trois mutations de pointe, dont F486R, N487R et Y489R. Résistance aux anticorps Une pression de sélection d'anticorps a été appliquée à la souche WA-1 pour identifier les mutations potentielles d'échappement qui peuvent apparaître au cours de l'infection virale. La pression de sélection positive a été appliquée en incubant le virus avec des concentrations croissantes des anticorps pour déclencher la résistance aux anticorps. Dans deux des anticorps les plus puissants, l'un était affecté négativement par une seule mutation F486S et l'autre était affecté par les mutations F486L, N487D et Q493R. Cependant, la mutation Q493R a montré un impact négligeable sur la liaison et la neutralisation. Une analyse plus poussée a révélé que ces mutations d'échappement sont principalement absentes dans les variantes virales circulantes, indiquant l'absence de pression de sélection. En effectuant plusieurs cycles de sélection à l'aide de traitements combinés avec deux anticorps, il a été observé que les combinaisons d'anticorps pourraient réduire le risque d'acquisition de mutations d'échappement et le développement ultérieur de variantes virales résistantes. Source: News Medical et merci à QcLiLi, dans Twitter En référence à "Wang L. 2021. Anticorps ultrapuissants contre des variantes diverses et hautement transmissibles du SRAS-CoV-2. Sciences". -- -- --
Virus entry, consisting of attachment to and penetration into the host target cell, is the first step of the virus life cycle and is a critical ‘do or die’ event that governs virus emergence in host populations. Most antiviral vaccines induce neutralizing antibodies that prevent virus entry into cells. However, while the prevention of virus invasion by humoral immunity is well appreciated, considerably less is known about the immune defences present within cells (known as intrinsic immunity) that interfere with virus entry. The interferon-induced transmembrane (IFITM) proteins, known for inhibiting fusion between viral and cellular membranes, were once the only factors known to restrict virus entry. However, the progressive development of genetic and pharmacological screening platforms and the onset of the COVID-19 pandemic have galvanized interest in how viruses infiltrate cells and how cells defend against it. Several host factors with antiviral potential are now implicated in the regulation of virus entry, including cholesterol 25-hydroxylase (CH25H), lymphocyte antigen 6E (LY6E), nuclear receptor co-activator protein 7 (NCOA7), interferon-γ-inducible lysosomal thiol reductase (GILT), CD74 and ARFGAP with dual pleckstrin homology domain-containing protein 2 (ADAP2). This Review summarizes what is known and what remains to be understood about the intrinsic factors that form the first line of defence against virus infection. Besides neutralizing antibodies, viruses face a range of cell-intrinsic inhibitors that are specialized to limit virus entry into host cells. Majdoul and Compton describe the mechanisms of action of the cellular factors providing this important first line of defence against virus infection, including infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The introduction of vaccines has inspired new hope in the battle against SARS-CoV-2. However, the emergence of viral variants, in the absence of potent antivirals, has left the world struggling wit...
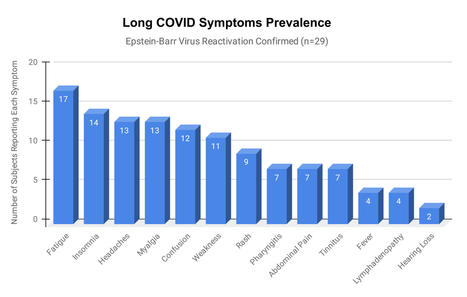
Epstein-Barr virus (EBV) reactivation resulting from the inflammatory response to coronavirus infection may be the cause of previously unexplained long COVID symptoms—such as fatigue, brain fog, and rashes—that occur in approximately 30% of patients after recovery from initial COVID-19 infection. The first evidence linking EBV reactivation to long COVID, as well as an analysis of long COVID prevalence, is outlined in a new long COVID study published in the journal Pathogens. "We ran EBV antibody tests on recovered COVID-19 patients, comparing EBV reactivation rates of those with long COVID symptoms to those without long COVID symptoms," said lead study author Jeffrey E. Gold of World Organization. "The majority of those with long COVID symptoms were positive for EBV reactivation, yet only 10% of controls indicated reactivation." The researchers began by surveying 185 randomly selected patients recovered from COVID-19 and found that 30.3% had long term symptoms consistent with long COVID after initial recovery from SARS-CoV-2 infection. This included several patients with initially asymptomatic COVID-19 cases who later went on to develop long COVID symptoms.
The researchers then found, in a subset of 68 COVID-19 patients randomly selected from those surveyed, that 66.7% of long COVID subjects versus 10% of controls were positive for EBV reactivation based on positive EBV early antigen-diffuse (EA-D) IgG or EBV viral capsid antigen (VCA) IgM titers. The difference was significant (p < 0.001, Fisher's exact test). "We found similar rates of EBV reactivation in those who had long COVID symptoms for months, as in those with long COVID symptoms that began just weeks after testing positive for COVID-19," said coauthor David J. Hurley, Ph.D., a professor and molecular microbiologist at the University of Georgia. "This indicated to us that EBV reactivation likely occurs simultaneously or soon after COVID-19 infection." The relationship between SARS-CoV-2 and EBV reactivation described in this study opens up new possibilities for long COVID diagnosis and treatment. The researchers indicated that it may be prudent to test patients newly positive for COVID-19 for evidence of EBV reactivation indicated by positive EBV EA-D IgG, EBV VCA IgM, or serum EBV DNA tests. If patients show signs of EBV reactivation, they can be treated early to reduce the intensity and duration of EBV replication, which may help inhibit the development of long COVID. "As evidence mounts supporting a role for EBV reactivation in the clinical manifestation of acute COVID-19, this study further implicates EBV in the development of long COVID," said Lawrence S. Young, Ph.D., a virologist at the University of Warwick, and Editor-in-Chief of Pathogens. "If a direct role for EBV reactivation in long COVID is supported by further studies, this would provide opportunities to improve the rational diagnosis of this condition and to consider the therapeutic value of anti-herpesvirus agents such as ganciclovir."
Original findings published in Pathogens (June 10, 2021):
L’infection par le virus d’Epstein-Barr peut être une des causes de longs symptômes de COVID tes que : la fatigue, les éruptions cutanées …
Cela permettrait de traiter tôt les patients afin de réduire l’intensité et la durée de la réplication de l’EBV, ce qui peut aider à inhiber le développement d'un long COVID.
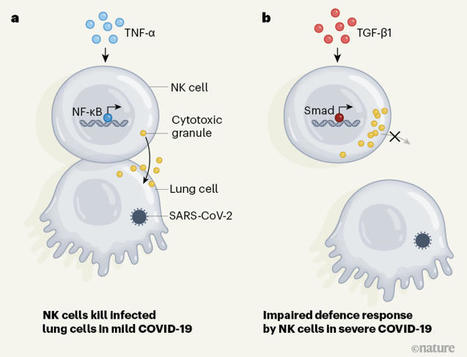
The release of neutrophil extracellular traps (NETs), a process termed NETosis, avoids pathogen spread but may cause tissue injury. NETs have been found in severe COVID-19 patients, but their role in disease development is still unknown. The aim of this study is to assess the capacity of NETs to drive epithelial-mesenchymal transition (EMT) of lung epithelial cells and to analyze the involvement of NETs in COVID-19. Bronchoalveolar lavage fluid of severe COVID-19 patients showed high concentration of NETs that correlates with neutrophils count; moreover, the analysis of lung tissues of COVID-19 deceased patients showed a subset of alveolar reactive pneumocytes with a co-expression of epithelial marker and a mesenchymal marker, confirming the induction of EMT mechanism after severe SARS-CoV2 infection. By airway in vitro models, cultivating A549 or 16HBE at air-liquid interface, adding alveolar macrophages (AM), neutrophils and SARS-CoV2, we demonstrated that to trigger a complete EMT expression pattern are necessary the induction of NETosis by SARS-CoV2 and the secretion of AM factors (TGF-β, IL8 and IL1β). All our results highlight the possible mechanism that can induce lung fibrosis after SARS-CoV2 infection.
In this study, we found that patients suffering from severe COVID-19 presented with immature, activated blood neutrophils and were characterized by elevated plasma levels of G-CSF and CXCL8 tha
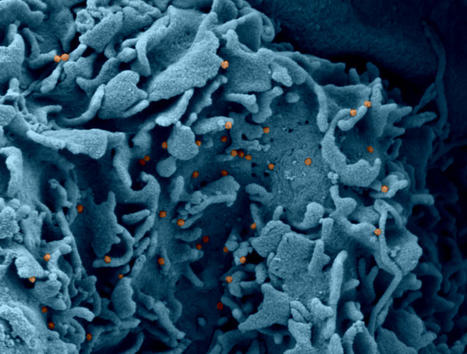
People who recover from mild COVID-19 have bone-marrow cells that can churn out antibodies for decades, though viral variants could dampen some of the protection they offer.
The zoonotic SARS-CoV-2 virus that causes COVID-19 continues to spread worldwide, with devastating consequences. While the medical community has gaine…
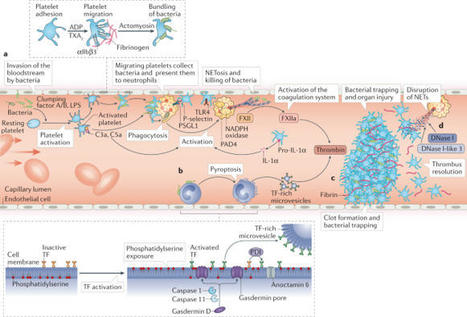
Thrombosis is the most feared complication of cardiovascular diseases and a main cause of death worldwide, making it a major health-care challenge. Platelets and the coagulation cascade are effectively targeted by antithrombotic approaches, which carry an inherent risk of bleeding. Moreover, antithrombotics cannot completely prevent thrombotic events, implicating a therapeutic gap due to a third, not yet adequately addressed mechanism, namely inflammation. In this Review, we discuss how the synergy between inflammation and thrombosis drives thrombotic diseases. We focus on the huge potential of anti-inflammatory strategies to target cardiovascular pathologies. Findings in the past decade have uncovered a sophisticated connection between innate immunity, platelet activation and coagulation, termed immunothrombosis. Immunothrombosis is an important host defence mechanism to limit systemic spreading of pathogens through the bloodstream. However, the aberrant activation of immunothrombosis in cardiovascular diseases causes myocardial infarction, stroke and venous thromboembolism. The clinical relevance of aberrant immunothrombosis, referred to as thromboinflammation, is supported by the increased risk of cardiovascular events in patients with inflammatory diseases but also during infections, including in COVID-19. Clinical trials in the past 4 years have confirmed the anti-ischaemic effects of anti-inflammatory strategies, backing the concept of a prothrombotic function of inflammation. Targeting inflammation to prevent thrombosis leaves haemostasis mainly unaffected, circumventing the risk of bleeding associated with current approaches. Considering the growing number of anti-inflammatory therapies, it is crucial to appreciate their potential in covering therapeutic gaps in cardiovascular diseases. In this Review, Stark and Massberg discuss how the interplay between innate immunity, platelet activation and coagulation, known as immunothrombosis, functions as a host defence mechanism to limit pathogen spreading, yet its aberrant activation, termed thromboinflammation, results in thrombotic complications, highlighting the therapeutic potential of anti-inflammatory strategies in cardiovascular pathologies.
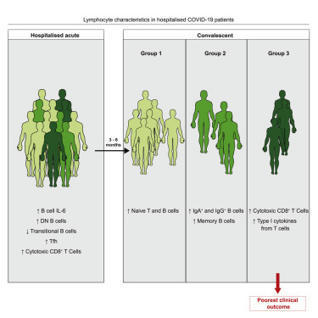
Une étude montre qu’il existe au moins deux profils de réponse cytokinique associée à la Covid-19, ce qui impliquerait donc la nécessité d’une prise en charge hautement personnalisée des patients.
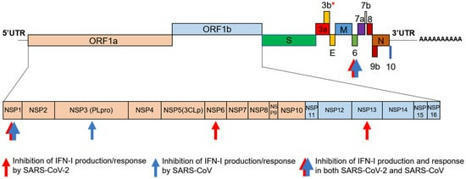
The global emergence of SARS-CoV-2 urgently requires an in-depth understanding of molecular functions of viral proteins and their interactions with the host proteome. Several individual omics studies have extended our knowledge of COVID-19 pathophysiology1–10. Integration of such datasets to obtain a holistic view of virus-host interactions and to define the pathogenic properties of SARS-CoV-2 is limited by the heterogeneity of the experimental systems. We therefore conducted a concurrent multi-omics study of SARS-CoV-2 and SARS-CoV. Using state-of-the-art proteomics, we profiled the interactome of both viruses, as well as their influence on transcriptome, proteome, ubiquitinome and phosphoproteome in a lung-derived human cell line. Projecting these data onto the global network of cellular interactions revealed crosstalk between the perturbations taking place upon SARS-CoV-2 and SARS-CoV infections at different layers and identified unique and common molecular mechanisms of these closely related coronaviruses. The TGF-β pathway, known for its involvement in tissue fibrosis, was specifically dysregulated by SARS-CoV-2 ORF8 and autophagy by SARS-CoV-2 ORF3. The extensive dataset (available at https://covinet.innatelab.org
) highlights many hotspots that can be targeted by existing drugs and it can guide rational design of virus- and host-directed therapies, which we exemplify by identifying kinase and MMPs inhibitors with potent antiviral effects against SARS-CoV-2.
Among the many activities attributed to the type I interferon (IFN) multigene family, their roles as mediators of the antiviral immune response have emerged as important components of the host response to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection.
COVID-19 can involve persistence, sequelae, and other medical complications that last weeks to months after initial recovery. This systematic review and meta-analysis aims to identify studies assessing the long-term effects of COVID-19. LitCOVID and Embase were searched to identify articles with original data published before the 1st of January 2021, with a minimum of 100 patients. For effects reported in two or more studies, meta-analyses using a random-effects model were performed using the MetaXL software to estimate the pooled prevalence with 95% CI. PRISMA guidelines were followed. A total of 18,251 publications were identified, of which 15 met the inclusion criteria. The prevalence of 55 long-term effects was estimated, 21 meta-analyses were performed, and 47,910 patients were included (age 17–87 years). The included studies defined long-COVID as ranging from 14 to 110 days post-viral infection. It was estimated that 80% of the infected patients with SARS-CoV-2 developed one or more long-term symptoms. The five most common symptoms were fatigue (58%), headache (44%), attention disorder (27%), hair loss (25%), and dyspnea (24%). Multi-disciplinary teams are crucial to developing preventive measures, rehabilitation techniques, and clinical management strategies with whole-patient perspectives designed to address long COVID-19 care.
Abstract Autopsies of patients who have died from COVID-19 have been crucial in delineating patterns of injury associated with SARS-CoV-2 infection. Despite their utility, comprehensive autopsy stu...
In collaboration with BioRender, Akiko Iwasaki, Ph.D., Professor of Immunobiology at Yale University School of Medicine, explores COVID-19 Immunology 101 for Non-immunologists.
Acknowledgements: Dr. Akiko Iwasaki, PhD (Collaborator, narrator, content expert) Dr. Yanet Valdez Tejeira, PhD (Spanish subtitle contributor) Mahadi B. Alyami (@RTKase) (Arabic subtitle contributor) Nick Atanelov (@Nick_atanelov) (Georgian subtitle contributor) Anonymous (Turkish subtitle contributor)
You can find and customize the figures used in this video by visiting the BioRender template library (http://app.biorender.com/biorender-templates) and search for "tweetorial".
About BioRender: BioRender is the easy-to-use science illustration tool that’s quickly becoming a staple in academic institutions and labs around the world! You can access the program for free at https://biorender.com/
Lowery et al. review the mechanisms by which SARS-CoV-2 activates and antagonizes the interferon and inflammatory response following infection, how a dysregulated cytokine and cellular response contributes to immune-mediated pathology in COVID-19, and therapeutic strategies that target elements of the innate response.
Title: COVID-19 and your immune system Date/Time: Tuesday 4 May 2021 – 18:00 to 19:00 Location: GoToWebinar Register now Description: The UK Coronavirus Immuno...
Emerging studies indicate that some coronavirus disease 2019 (COVID-19) patients suffer from persistent symptoms, including breathlessness and chronic…
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.



 Your new post is loading...
Your new post is loading...