Your new post is loading...
Your new post is loading...

|
Scooped by
Gilbert C FAURE
April 3, 7:10 AM
|
“Administered together with first-line TB drug therapy, our intranasal DNA fusion vaccine helped infected mice clear the disease bacteria faster, reduced lung inflammation and prevented relapse after treatment ended,” says study lead author Styliani Karanika, M.D., a faculty member of the Johns Hopkins Center for Tuberculosis Research and assistant professor of medicine at the Johns Hopkins University School of Medicine.
“The vaccine also helped the powerful TB drug combination of bedaquiline, pretomanid and linezolid work better, suggesting it could be used with treatments against drug-resistant TB to help the body fight the disease, even hard-to-treat cases.”
#intranasalTBvaccine
Vaccines and Immunology: A Foundation of Preventive Medicine
One of the most impactful applications of immunology is vaccination—a concept built on a simple yet powerful idea: training the immune system before exposure to disease.
The adaptive immune system’s ability to develop long-term memory allows vaccines to provide lasting protection with minimal risk. This principle has transformed global health outcomes and continues to shape modern medical innovation.
What’s particularly remarkable is how advancements in biotechnology—especially mRNA platforms—have accelerated vaccine development timelines without compromising safety or efficacy.
Vaccination is not only an individual health decision; it is a collective responsibility that strengthens public health systems through herd immunity.
As science continues to evolve, the role of immunology in preventive medicine will only become more critical.
The future of healthcare is not just about treating disease—but preventing it.
#Leadership #HealthcareInnovation #Vaccines #Immunology #FutureOfMedicine
|
|
Scooped by
Gilbert C FAURE
March 25, 2:31 PM
|
The most critical strategy for controlling the spread of infectious diseases is vaccination—making vaccine production processes pivotal to disease control and eventual eradication. Vaccination is an artificial process where inactivated, attenuated infectious pathogens, or their components, are delivered to the human body, using antigenic structures to activate the immune system. This process stimulates an effective response against specific pathogens to combat impending infections.
Since the mid-20th century, viral vaccines have been produced using chicken embryos, with dozens of approved traditional human vaccines manufactured via embryo-based processes. Today, however, cell culture-based vaccine production has become widespread: it enables simple infection and replication in controlled environments, with harvesting steps conducted in closed bioreactor systems to ensure sterility and further reduce biosafety risks through automation. This approach significantly boosts factory capacity, enabling the production of large quantities of vaccine doses.
|
|
Scooped by
Gilbert C FAURE
March 23, 2:44 AM
|
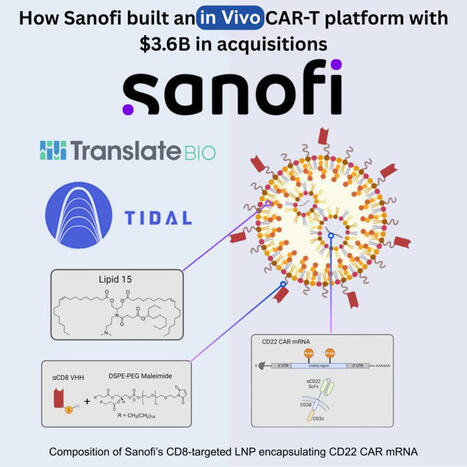
Sanofi just published their in vivo CAR-T data.
The paper will be published in 𝘔𝘰𝘭𝘦𝘤𝘶𝘭𝘢𝘳 𝘛𝘩𝘦𝘳𝘢𝘱𝘺 this month.
Was this built in-house? Not really. It's the result of two strategic acquisitions that tell you exactly how big pharma is entering in vivo cell engineering.
Everything started about 8 years ago with Sanofi entering the mRNA therapeutics space first.
In 2018, Sanofi partnered with Translate Bio for mRNA vaccines. $45M upfront. Focusing specifically on up to five infectious diseases.
COVID hit.
They expanded the deal in 2020 to $300M cash + $125M as stock investment, covering all infectious diseases.
Then in August 2021, they acquired the whole company for $3.2B!!!
What did they get? One of the largest private LNP libraries in the industry. mRNA manufacturing expertise. A platform ready to go beyond vaccines.
𝘉𝘶𝘵 𝘮𝘙𝘕𝘈 𝘵𝘦𝘤𝘩 𝘢𝘭𝘰𝘯𝘦 𝘥𝘰𝘦𝘴𝘯'𝘵 𝘮𝘢𝘬𝘦 𝘪𝘯 𝘷𝘪𝘷𝘰 𝘊𝘈𝘙-𝘛 𝘸𝘰𝘳𝘬!
Three months before closing Translate Bio, Sanofi acquired Tidal Therapeutics in April 2021. $160M upfront, $470M total including milestones.
𝗦𝗮𝗻𝗼𝗳𝗶'𝘀 𝘁𝗼𝘁𝗮𝗹 𝗰𝗼𝗺𝗺𝗶𝘁𝗺𝗲𝗻𝘁:
+$𝟯.𝟲𝗕 𝘁𝗼 𝗲𝗻𝘁𝗲𝗿 𝘁𝗵𝗲 𝗺𝗥𝗡𝗔 𝗮𝗻𝗱 𝗶𝗻 𝘃𝗶𝘃𝗼 𝗖𝗔𝗥-𝗧 𝘀𝗽𝗮𝗰𝗲
Tidal brought the missing piece: targeted nanoparticle technology to reprogram immune cells directly in the body.
Now the paper shows what happens when you combine both platforms.
The technical execution is solid:
• Proprietary ionizable lipid 15 for T cell transfection
• Anti-CD8 VHH nanobody outperforming other ligands
• CD22 CAR benchmarked against clinically validated CARs (FMC63 and m971)
• Hepatic de-targeting, under 5% liver uptake
• Tumor suppression in aggressive human models
That last point matters. Getting mRNA into T cells is hard enough.
Keeping it away from liver trapping while maintaining efficacy is the real challenge.
They solved both.
This is how platforms get built in 2025. You don't develop everything internally. You acquire the best technology, integrate it fast, and publish validation data within a few years.
Translate Bio gave them the mRNA engine. Tidal gave them the targeting system. Together, they created an in vivo CAR-T platform neither could build alone.
The question now is whether improvements we witness in the in vivo CAR-T space will scale beyond hematological malignancies.
The delivery is transient.
The safety profile looks clean (mRNA).
Serial killing durability up to 8 days.
And repeat dosing gave no signs of toxicity.
Can this match the persistence of ex vivo products?
Will in vivo CAR-T platforms ever be efficacious in solid tumors?
So much money has been invested in this tech and we are seeing progress with creative solutions to optimize in vivo CAR-T platforms.
Pre-print link to the article in the comments!
-----------------------------------------------------------
I share insights on all things xRNA, CAR-X and CGT innovation. Follow me for more biotech insights | 33 comments on LinkedIn
|
|
Scooped by
Gilbert C FAURE
March 21, 6:37 AM
|
|
|
Scooped by
Gilbert C FAURE
March 20, 11:28 AM
|
This week’s Global Health Notes looks at how science and policy are shaping disease prevention — from vaccine‑carrying mosquitoes and India’s HPV rollout to new ways countries plan and fund vaccines.
|
|
Scooped by
Gilbert C FAURE
March 18, 6:04 AM
|
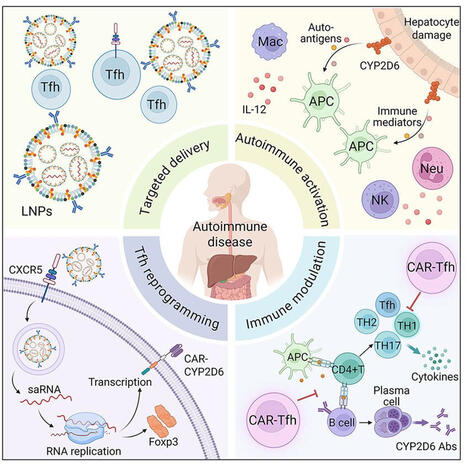
Interesting in Cell Stem Cell: In vivo CAR-Tfh cell reprogramming restores tolerance in a mouse model of autoimmune hepatitis
https://lnkd.in/en36DGSU
Autoimmune diseases involve the coordinated dysregulation of multiple types of immune cells, and single-cell targeted therapies often yield suboptimal results. Here, we developed chimeric antigen receptor (CAR)-engineered follicular helper T (Tfh) cells capable of simultaneously suppressing T cells, B cells, and dendritic cells (DCs) to restore immune homeostasis in an autoimmune hepatitis (AIH) mouse model. Using amino acid-derived lipid nanoparticles, we deliver self-amplifying RNA encoding Forkhead box protein P3 (Foxp3) and a cytochrome P4502D6 (CYP2D6)-specific CAR to Tfh cells, conferring stable regulatory features and antigen-dependent suppressive activity. Engineered CAR-Tfh cells preferentially localize to the liver, recognize CYP2D6-expressing hepatocytes, and suppress pathogenic T cell and B cell responses. In AIH-II mouse models, CAR-Tfh cell generation restores a tolerogenic hepatic immune environment and ameliorates autoimmune liver injury. These findings establish in situ Tfh cell reprogramming as a modular approach to coordinately modulate multiple immune compartments, providing a potential therapeutic framework for AIH and related autoimmune diseases.
|
|
Scooped by
Gilbert C FAURE
March 16, 5:49 AM
|
🔬 Recent Trends in Vaccine Delivery Systems: Transforming Modern Immunization
Vaccines remain one of the most powerful tools in preventive medicine, protecting millions of lives each year.
While traditional vaccines have been highly effective, modern science is now focusing on innovative vaccine delivery systems to improve immunogenicity, stability, and targeted immune responses.
Here are some important advancements shaping the future of vaccination:
🧬 1. Subunit and Recombinant Vaccines
Instead of using whole pathogens, these vaccines use specific antigenic components such as proteins or polysaccharides.
✔ Higher safety profile
✔ Targeted immune response
✔ Reduced adverse reactions
However, these vaccines often require adjuvants to enhance immune stimulation.
💉 2. Advanced Vaccine Delivery Platforms
Modern delivery systems are being designed to optimize antigen presentation and immune activation.
Key technologies include:
• Liposomes – Lipid-based vesicles that encapsulate antigens and improve immune recognition
• Microparticles / Nanoparticles – Controlled release systems that enhance antigen stability
• ISCOMs (Immune Stimulating Complexes) – Improve antigen uptake by antigen-presenting cells
• Emulsion-based delivery systems – Facilitate sustained antigen release
These technologies help ensure better immune activation with lower antigen doses.
🧪 3. Role of Adjuvants
Adjuvants play a critical role in vaccine effectiveness by:
✔ Enhancing immune response
✔ Promoting long-lasting immunity
✔ Reducing the amount of antigen required
They function by stimulating pattern recognition receptors (PRRs) of the innate immune system, thereby strengthening adaptive immune responses.
🌍 Why This Matters
The development of advanced vaccine delivery systems is critical for:
• Emerging infectious diseases
• Pandemic preparedness
• Cancer immunotherapy
• Chronic viral infections such as hepatitis
These innovations are helping us move toward safer, more effective, and more targeted immunization strategies.
💡 Key Takeaway
The future of vaccination is not just about the antigen itself, but also about how it is delivered to the immune system.
Modern delivery platforms and adjuvants are revolutionizing vaccine science and opening new possibilities for global disease prevention.
🔗 Let’s continue advancing collaborative research in microbiology, immunology, and pharmaceutical sciences to strengthen global health security.
#Vaccines #Immunology #Microbiology #PharmaceuticalScience #PublicHealth #DrugDelivery #BiomedicalResearch #InfectiousDiseases #HealthcareInnovation
|
|
Scooped by
Gilbert C FAURE
March 14, 6:02 AM
|
Gostaria de compartilhar o artigo “A segurança e a inovação de vacinas no Brasil”, publicado na seção Tendências/Debates, na edição de 1° de março no jornal “Folha de S. Paulo", do qual sou co-autor.
O texto discute um ponto central para o futuro da saúde no país: como equilibrar proteção regulatória, ética e agilidade para permitir que a inovação nacional floresça.
Embora o Brasil possua instituições regulatórias sólidas, ainda enfrentamos desafios estruturais que impactam diretamente a competitividade científica e tecnológica. A morosidade e a assimetria regulatória acabam favorecendo grandes players internacionais e dificultando o avanço de vacinas concebidas e desenvolvidas no país.
A pandemia deixou clara a importância da soberania tecnológica em saúde. Fortalecer o ecossistema nacional de inovação exige não apenas financiamento, mas também um ambiente regulatório moderno, previsível e adaptativo.
A recente Lei 14.874/2025 e iniciativas de acompanhamento regulatório representam passos importantes. O desafio agora é transformar expectativa em implementação efetiva.
Seguimos trabalhando para que ciência, ética e desenvolvimento caminhem juntos — com protagonismo brasileiro.
https://lnkd.in/dhJ7cJg2
#Inovação #Vacinas #SaúdePública #SoberaniaTecnológica #Regulação #CiênciaBrasileira
|
|
Scooped by
Gilbert C FAURE
March 12, 5:05 AM
|
Researchers at Virginia Tech are developing a new class of #vaccines designed to block #opioids from reaching the #brain - an approach that could help address the ongoing #overdose crisis in the United States.
▫️ In a study published in the Journal of Controlled Release, a team led by Chenming Zhang , professor and Turner Faculty Fellow in the Department of Biological Systems Engineering, created a hybrid lipid-polymer #nanoparticle #vaccine that triggered stronger #immuneresponses and improved protection against #oxycodone in mice. The work was supported by The National Institutes of Health and involved contributions from undergraduate researcher Kari Cochran from the Virginia Tech College of Engineering.
▫️The vaccine uses biodegradable nanoparticles that mimic viruses in size and structure, prompting the #immunesystem to produce #antibodies that bind to opioid molecules such as oxycodone or #fentanyl. By preventing these drugs from crossing the blood–brain barrier, the approach blocks the euphoric effects that drive addiction while still allowing other medical treatments to function normally.
▫️Early findings suggest the antibodies remain active for months and could potentially be optimized to provide year-long protection. While not intended for general vaccination, the strategy could be used for individuals with opioid use disorder or those at high risk of exposure.
💡 If successful, this research could open a new frontier where vaccines are used not only to prevent #infectiousdiseases but also to address chronic conditions like #addiction, potentially reducing overdose deaths and supporting recovery.
🗃️ See comments for reference.
|
|
Scooped by
Gilbert C FAURE
March 9, 5:47 AM
|
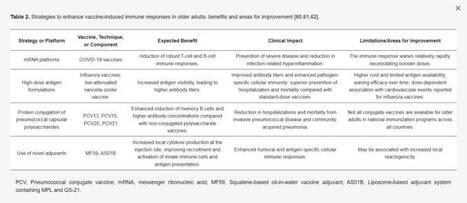
The remodeling of the immune system with age has significant implications for public health. Vaccines that are highly effective in children and young adults often elicit weaker responses in older adults, resulting in reduced protection. This challenge has spurred the development of new strategies, including high-dose formulations, vaccines with novel adjuvants that enhance antigen presentation, and antigen conjugation technologies that improve immunogenicity.
https://lnkd.in/dybunHnu
|
|
Scooped by
Gilbert C FAURE
February 20, 2:02 AM
|
𝗧𝗿𝗶𝗸𝗶𝗻𝗲𝘀: 𝗔𝗡𝗗-𝗴𝗮𝘁𝗲𝗱 𝗰𝘆𝘁𝗼𝗸𝗶𝗻𝗲𝘀 𝘁𝗼 𝗿𝗲𝗽𝗿𝗼𝗴𝗿𝗮𝗺 𝗦𝗧𝗔𝗧 𝘀𝗶𝗴𝗻𝗮𝗹𝗶𝗻𝗴
🧠 𝗔 𝗽𝗮𝗽𝗲𝗿 𝗮 𝗱𝗮𝘆 𝗸𝗲𝗲𝗽𝘀 𝗯𝗿𝗮𝗶𝗻 𝗱𝗲𝗰𝗮𝘆 𝗮𝘄𝗮𝘆 🧠
Friday 20 February 2026
𝘛𝘳𝘪𝘬𝘪𝘯𝘦𝘴 𝘢𝘳𝘦 𝘦𝘯𝘨𝘪𝘯𝘦𝘦𝘳𝘦𝘥 𝘤𝘺𝘵𝘰𝘬𝘪𝘯𝘦𝘴 𝘵𝘩𝘢𝘵 𝘧𝘰𝘳𝘤𝘦 𝘵𝘩𝘳𝘦𝘦-𝘤𝘩𝘢𝘪𝘯 𝘳𝘦𝘤𝘦𝘱𝘵𝘰𝘳 𝘢𝘴𝘴𝘦𝘮𝘣𝘭𝘺 𝘵𝘰 𝘤𝘳𝘦𝘢𝘵𝘦 𝘈𝘕𝘋-𝘨𝘢𝘵𝘦𝘥, 𝘯𝘰𝘯-𝘯𝘢𝘵𝘶𝘳𝘢𝘭 𝘚𝘛𝘈𝘛 𝘴𝘪𝘨𝘯𝘢𝘭𝘪𝘯𝘨 𝘱𝘳𝘰𝘨𝘳𝘢𝘮𝘴 𝘸𝘪𝘵𝘩𝘪𝘯 𝘴𝘪𝘯𝘨𝘭𝘦 𝘤𝘦𝘭𝘭𝘴, 𝘦𝘯𝘢𝘣𝘭𝘪𝘯𝘨 𝘱𝘳𝘦𝘤𝘪𝘴𝘦 𝘪𝘮𝘮𝘶𝘯𝘦 𝘢𝘤𝘵𝘪𝘷𝘢𝘵𝘪𝘰𝘯 𝘸𝘩𝘪𝘭𝘦 𝘱𝘳𝘦𝘴𝘦𝘳𝘷𝘪𝘯𝘨 𝘛-𝘤𝘦𝘭𝘭 𝘴𝘵𝘦𝘮𝘯𝘦𝘴𝘴 𝘢𝘯𝘥 𝘳𝘦𝘥𝘶𝘤𝘪𝘯𝘨 𝘴𝘺𝘴𝘵𝘦𝘮𝘪𝘤 𝘵𝘰𝘹𝘪𝘤𝘪𝘵𝘺 𝘸𝘪𝘵𝘩𝘰𝘶𝘵 𝘨𝘦𝘯𝘦𝘵𝘪𝘤 𝘦𝘯𝘨𝘪𝘯𝘦𝘦𝘳𝘪𝘯𝘨.
💡𝗧𝗮𝗸𝗲 𝗵𝗼𝗺𝗲 𝗺𝗲𝘀𝘀𝗮𝗴𝗲
• IL-2/21 and IL-10/2 Trikines fuse a cytokine with a receptor-binding module to recruit a third receptor chain in cis, forming tri-receptor complexes that reprogram intracellular STAT signaling within the same cell.
• IL-2/21 Trikine enforces IL-2Rβ/γc and IL-21Rα co-engagement, generating pSTAT5 with IL-21-like pSTAT3, preserving stem-like CD8 T cells, limiting exhaustion, enhancing tumor control, and avoiding IL-2–driven NK toxicity.
• IL-10/2 Trikine adds IL-2Rβ–STAT5 signaling to IL-10–driven STAT3, boosting tumor infiltration and, with PD-1 blockade, expanding cycling TILs to suppress refractory lung and pancreatic tumors.
🔥𝗜𝗺𝗽𝗮𝗰𝘁
• AND-gated Trikines could replace cytokine cocktails and cell engineering, delivering tunable STAT programs with reduced systemic toxicity to overcome immunosuppression in solid tumors.
❓𝗢𝗽𝗲𝗻 𝗾𝘂𝗲𝘀𝘁𝗶𝗼𝗻𝘀
• Which receptor-density thresholds best predict Trikine responsiveness across exhausted, stem-like, and regulatory T-cell states?
• Can modular Trikine architectures successfully decouple and exploit other pleiotropic profiles like STAT1/STAT4 pathways?
• Will human-reactive Trikines mirror murine pharmacokinetics and sustain patient TIL stemness during clinical translation
𝗥𝗲𝘄𝗶𝗿𝗶𝗻𝗴 𝗦𝗧𝗔𝗧 𝘀𝗶𝗴𝗻𝗮𝗹𝗶𝗻𝗴 𝗳𝗿𝗼𝗺 𝘁𝗵𝗲 𝗰𝗲𝗹𝗹 𝘀𝘂𝗿𝗳𝗮𝗰𝗲 𝘄𝗶𝘁𝗵 𝗧𝗿𝗶𝗸𝗶𝗻𝗲 𝗶𝗺𝗺𝘂𝗻𝗼𝘁𝗵𝗲𝗿𝗮𝗽𝗲𝘂𝘁𝗶𝗰𝘀
Grayson E. Rodriguez, Yang Zhao et al
Science, February 2026
Corresponding author: K. Christopher Garcia
🔗 𝘓𝘪𝘯𝘬 𝘵𝘰 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤𝘢𝘵𝘪𝘰𝘯 𝘪𝘯 𝘤𝘰𝘮𝘮𝘦𝘯𝘵𝘴
𝘐𝘭𝘭𝘶𝘴𝘵𝘳𝘢𝘵𝘪𝘰𝘯 𝘢𝘥𝘢𝘱𝘵𝘦𝘥 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘢𝘳𝘵𝘪𝘤𝘭𝘦.
𝘛𝘩𝘦 𝘰𝘱𝘪𝘯𝘪𝘰𝘯𝘴 𝘴𝘩𝘢𝘳𝘦𝘥 𝘰𝘯 𝘓𝘪𝘯𝘬𝘦𝘥𝘐𝘯 𝘢𝘳𝘦 𝘮𝘺 𝘰𝘸𝘯.
|
|
Scooped by
Gilbert C FAURE
February 16, 2:05 AM
|
End-stage organ failure requires the transplantation of a new organ. However, the number of patients awaiting donor organs exceeds the number of available organs. To address this organ shortage, solid organs, such as the kidneys, liver, heart and lungs, can be engineered based on decellularized human and non-human tissues. These decellularized scaffolds can then be recellularized with autologous or allogeneic cells and modified to ensure engraftment and function following transplantation. In this Review, we discuss the creation of decellularized neo-solid organs, including animal donor considerations, pre-decellularization processes, decellularization protocols, post-decellularization characterization, sterilization and storage conditions. We highlight various cell seeding and modification strategies and examine bioreactor culture conditions to grow functional solid organs. Finally, we outline mechanisms of transplant-recipient crosstalk and discuss challenges and opportunities for the clinical translation of engineered solid organs. New organs can be engineered based on decellularized human and animal tissues to address the global shortage of donor organs. This Review discusses design principles for the engineering of new organs using decellularized animal-derived tissues, including decellularization, functionalization and characterization protocols.
|
|
|
Scooped by
Gilbert C FAURE
April 1, 3:34 AM
|
𝐓𝐨𝐩 𝐂𝐨𝐦𝐩𝐚𝐧𝐢𝐞𝐬 𝐢𝐧 𝐕𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐈𝐧𝐝𝐮𝐬𝐭𝐫𝐲
𝐃𝐨𝐰𝐧𝐥𝐨𝐚𝐝 𝐏𝐃𝐅 𝐁𝐫𝐨𝐜𝐡𝐮𝐫𝐞: https://lnkd.in/dFNjk8eY
The global vaccines market (excluding COVID-19 vaccines), valued at USD 49.59 billion in 2024, stood at USD 47.65 billion in 2025 and is projected to advance at a resilient CAGR of 7.3% from 2025 to 2030, culminating in a forecasted valuation of USD 67.91 billion by the end of the period.
The market is growing due to several factors, including the rapid development and global commercialization of vaccines, the increasing prevalence of infectious diseases that require vaccination for prevention, the rising number of immunization programs, advancements in technology that support vaccine development, and increased government support through investments and funding aimed at creating new vaccines for various disease indications.
• The North America vaccines market accounted for a 52.3% revenue share in 2024.
• By disease indication, the pneumococcal disease segment is expected to register the highest CAGR of 10.6%.
• By technology, the inactivated & subunit vaccines segment is projected to grow at the fastest rate from 2025 to 2030.
• By end user, the adult vaccines segment accounted for a larger share of 54.0% of the market in 2024.
• Companies such as GSK, Merck Group, Pfizer were identified as some of the star players in the vaccines market (global), given their strong market share and product footprint.
• Companies such as SINOVAC BIOTECH LTD., Incepta Pharmaceuticals Ltd., Valneva among others, have distinguished themselves among startups and SMEs by securing strong footholds in specialized niche areas, underscoring their potential as emerging market leaders
|
|
Scooped by
Gilbert C FAURE
March 25, 2:35 PM
|
🐄 Understanding Vaccination & Antibody Titre Dynamics in Dairy Cattle 🧬
Effective vaccination is not just about injecting vaccines—it’s about understanding how the immune system responds and how long protection lasts.
🔬 What happens after vaccination?
The animal’s immune system produces antibodies. The first response is slow and low, while booster doses create a faster and stronger immunity.
📊 Antibody Titre Dynamics:
Antibody levels follow a pattern:
➡️ Lag Phase → 📈 Peak → 📉 Decline
This is why timely booster doses are essential to maintain protection.
🐮 Maternal Antibodies in Calves:
- Obtained through colostrum
- Provide early protection
- Can interfere with early vaccination
⏳ Proper timing of vaccination in calves is critical to avoid vaccine failure.
📅 Practical Vaccination Strategy:
- Calves: 3–6 months
- Boosters: 2–4 weeks after first dose
- Adults: Annual or biannual vaccination
⚠️ Factors Affecting Immune Response:
- Nutrition (Protein, Zinc, Selenium)
- Stress & disease conditions
- Proper vaccine storage & handling (cold chain)
🧪 Why Antibody Titre Testing Matters?
- Evaluate vaccine effectiveness
- Monitor herd immunity
- Optimize vaccination programs
(Common method: ELISA)
💡 Key Takeaways:
✔ Boosters are critical
✔ Good nutrition improves immunity
✔ Monitor and adapt vaccination plans
🌱 Strong immunity = Healthy herd = Better productivity
#DairyFarming #HerdHealth #DairyNutrition
|
|
Scooped by
Gilbert C FAURE
March 24, 11:48 AM
|
The immune system can be your best friend for mRNA vaccines - and also your biggest bottleneck.
A new paper in npj Vaccines by Lobb et al., highlights a counterintuitive point: type I interferon (IFN), a key innate immune alarm signal, can reduce mRNA-LNP vaccine effectiveness if it’s triggered at the wrong time, because activated dendritic cells lose the ability to take up new antigen.
In their models, blocking IFNα/β receptor signaling before vaccination (or removing the receptor specifically in dendritic cells) increased vaccine uptake/expression in DCs, improved CD8⁺ T-cell priming, and led to better tumor control. They also show a practical implication: IFN already “in the system” (for example after an infection or a recent prior vaccination) can blunt the response to an mRNA-LNP vaccine given shortly afterwards.
This connects directly to a theme we care about at Sensible Biotechnologies: for mRNA medicines, purity and innate immune activation are not “nice-to-have” quality attributes - they can materially shape uptake, translation, and ultimately efficacy. If IFN signaling suppresses antigen acquisition and translation capacity in key antigen-presenting cells, then minimizing unnecessary innate triggers (including those driven by impurities) becomes part of the performance equation, not just the safety story.
That’s why Sensible is focused on maximizing mRNA purity and minimizing immunogenicity as we build a vertically integrated, cell-based platform for mRNA design and manufacturing.
Read the paper in npj Vaccines on the link below:
https://lnkd.in/dh46rrgy
#mrna #biotech #immunology #drugdevelopment
|
|
Scooped by
Gilbert C FAURE
March 21, 6:49 AM
|
From PK regulator to therapeutic breakthrough, FcRn is reshaping autoimmune treatment. With Vyvgart expanding into CIDP and Nipocalimab advancing in SLE and HDFN, the “chemical plasmapheresis” era is accelerating.
As FcRn programs grow, precise control of pH-dependent binding is essential for long-acting mAb design and clinical success.
ACROBiosystems supports FcRn innovation with:
✔ High-quality FcRn proteins
✔ TR-FRET binding kits
✔ Functional cell lines
Enable precision from discovery to IND.
👉 Advance your FcRn program with confidence.
|
|
Scooped by
Gilbert C FAURE
March 20, 12:17 PM
|
Il n'existe actuellement aucun traitement efficace contre l'insuffisance rénale aiguë, qui est associée à des longues hospitalisations et un taux de (…)
|
|
Scooped by
Gilbert C FAURE
March 18, 7:07 AM
|
𝗖𝗔𝗥-𝗧 𝗶𝗻 𝘀𝗼𝗹𝗶𝗱 𝘁𝘂𝗺𝗼𝗿𝘀 - 𝗮 𝗿𝗲𝘃𝗶𝗲𝘄
🧠 𝗔 𝗽𝗮𝗽𝗲𝗿 𝗮 𝗱𝗮𝘆 𝗸𝗲𝗲𝗽𝘀 𝗯𝗿𝗮𝗶𝗻 𝗱𝗲𝗰𝗮𝘆 𝗮𝘄𝗮𝘆 🧠
Monday 16 March 2026
𝘚𝘰𝘭𝘪𝘥 𝘵𝘶𝘮𝘰𝘳 𝘊𝘈𝘙-𝘛 𝘤𝘦𝘭𝘭 𝘵𝘩𝘦𝘳𝘢𝘱𝘺 𝘪𝘴 𝘴𝘵𝘢𝘳𝘵𝘪𝘯𝘨 𝘵𝘰 𝘨𝘦𝘯𝘦𝘳𝘢𝘵𝘦 𝘳𝘦𝘢𝘭 𝘤𝘭𝘪𝘯𝘪𝘤𝘢𝘭 𝘳𝘦𝘴𝘱𝘰𝘯𝘴𝘦𝘴, 𝘣𝘶𝘵 𝘥𝘶𝘳𝘢𝘣𝘭𝘦 𝘴𝘶𝘤𝘤𝘦𝘴𝘴 𝘸𝘪𝘭𝘭 𝘥𝘦𝘱𝘦𝘯𝘥 𝘰𝘯 𝘰𝘷𝘦𝘳𝘤𝘰𝘮𝘪𝘯𝘨 𝘢𝘯𝘵𝘪𝘨𝘦𝘯 𝘩𝘦𝘵𝘦𝘳𝘰𝘨𝘦𝘯𝘦𝘪𝘵𝘺, 𝘱𝘰𝘰𝘳 𝘵𝘳𝘢𝘧𝘧𝘪𝘤𝘬𝘪𝘯𝘨, 𝘰𝘯-𝘵𝘢𝘳𝘨𝘦𝘵 𝘰𝘧𝘧-𝘵𝘶𝘮𝘰𝘳 𝘵𝘰𝘹𝘪𝘤𝘪𝘵𝘺, 𝘢𝘯𝘥 𝘵𝘩𝘦 𝘴𝘶𝘱𝘱𝘳𝘦𝘴𝘴𝘪𝘷𝘦 𝘵𝘶𝘮𝘰𝘳 𝘮𝘪𝘤𝘳𝘰𝘦𝘯𝘷𝘪𝘳𝘰𝘯𝘮𝘦𝘯𝘵.
💡𝗧𝗮𝗸𝗲 𝗵𝗼𝗺𝗲 𝗺𝗲𝘀𝘀𝗮𝗴𝗲
• Clinical efficacy: While response rates in solid tumors remain modest overall, clear “pockets of promise” exist in neuroblastoma (GD2), sarcoma (HER2), and glioblastoma (IL-13Rα2), with some trials reporting complete response rates up to ~31%.
• Biological barriers: Major challenges include antigen heterogeneity, on-target off-tumor toxicity, poor T cell trafficking, and an immunosuppressive tumor microenvironment. The field is moving toward armored CARs (for example IL-12 or IL-15 secreting cells) and logic-gated circuits such as SynNotch to improve specificity and persistence.
• Manufacturing innovation: New ex vivo strategies — including metabolic priming with L-arginine and shortened vein-to-vein production (24–72 h) — aim to preserve T cell stemness and reduce exhaustion.
• Emerging platforms: Allogeneic “off-the-shelf” CAR-T products and in vivo CAR engineering using lipid nanoparticles are being explored to overcome scalability and manufacturing complexity.
🔥𝗜𝗺𝗽𝗮𝗰𝘁
• Future progress will likely come from integrated cell engineering and tumor-specific clinical strategies, not receptor design alone.
❓𝗢𝗽𝗲𝗻 𝗾𝘂𝗲𝘀𝘁𝗶𝗼𝗻𝘀
• Which antigen combinations best balance tumor coverage and safety?
• Which armored CAR payloads enhance efficacy without systemic toxicity?
• How should conditioning, delivery route, and combinations differ by tumor type?
𝗖𝘂𝗿𝗿𝗲𝗻𝘁 𝘀𝘁𝗮𝘁𝗲 𝗼𝗳 𝗖𝗔𝗥-𝗧 𝗰𝗲𝗹𝗹 𝘁𝗵𝗲𝗿𝗮𝗽𝗶𝗲𝘀 𝗳𝗼𝗿 𝘀𝗼𝗹𝗶𝗱 𝘁𝘂𝗺𝗼𝗿𝘀
Reginaldo Rosa, MBA, PhD et al.
Med, February 2026
Corresponding author: Saul Priceman
🔗 𝘓𝘪𝘯𝘬 𝘵𝘰 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤𝘢𝘵𝘪𝘰𝘯 𝘪𝘯 𝘤𝘰𝘮𝘮𝘦𝘯𝘵𝘴
𝘐𝘭𝘭𝘶𝘴𝘵𝘳𝘢𝘵𝘪𝘰𝘯 𝘢𝘥𝘢𝘱𝘵𝘦𝘥 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘢𝘳𝘵𝘪𝘤𝘭𝘦.
𝘛𝘩𝘦 𝘰𝘱𝘪𝘯𝘪𝘰𝘯𝘴 𝘴𝘩𝘢𝘳𝘦𝘥 𝘰𝘯 𝘓𝘪𝘯𝘬𝘦𝘥𝘐𝘯 𝘢𝘳𝘦 𝘮𝘺 𝘰𝘸𝘯.
| 11 comments on LinkedIn
|
|
Scooped by
Gilbert C FAURE
March 18, 4:04 AM
|
You’ve heard of CAR-T.
But you might not know about CAAR-T - a newer, more targeted twist on the same technology:
So what is it?
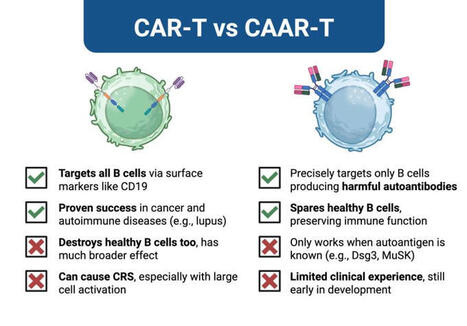
- CAAR-T (Chimeric AutoAntibody Receptor T cells) are designed to eliminate only the B cells producing harmful autoantibodies, while sparing the rest.
- Instead of using an antibody fragment to find targets (like CAR-T does), CAAR-T cells display an autoantigen on their surface, tricking autoreactive B cells into binding and revealing themselves.
Here’s how they compare:
CAR-T Cells
Advantages:
- Targets all B cells via markers like CD19
- Proven success in cancer and autoimmune diseases (e.g., lupus)
Disadvantages:
- Destroys healthy B cells too, leading to broader immune impact
- Can cause CRS, especially with large-scale immune activation
CAAR-T Cells
Advantages:
- Precisely targets only B cells producing harmful autoantibodies
- Spares healthy B cells, preserving immune function
Disadvantages:
- Requires known autoantigen (e.g., Dsg3, MuSK)
- Limited clinical experience, still early in development
In short:
CAR-T is broad and proven.
CAAR-T is precise and emerging.
Now, I don't see CAAR-T replacing CAR-T.
But for autoantibody-driven diseases, it could offer something we’ve never had before:
A precise strike against the root cause, without wiping out the entire immune arsenal.
Anything else you'd add?
Drop it in the comments. | 31 comments on LinkedIn
|
|
Scooped by
Gilbert C FAURE
March 14, 8:33 AM
|
Butantan Dengue Vaccine 81% Effective Against Severe Disease for 5 years -
The results of a phase 3 clinical trial of the Butanan vaccine are now published in Nature Medicine. The single-dose tetravalent dengue vaccine developed by Brazil’s Butantan Institute is 80.5% effective against hospitalization for the mosquito-borne disease for at least five years.
The double-blind, placebo-controlled trial included 10,259 vaccinated individuals and 5,976 in the placebo control.
Over five years, no vaccinated participants were hospitalized. VE against symptomatic dengue was 65.0%. VE was 77.1% in previously infected participants, 58.9% in dengue-naive participants, 73.0% against DENV-1, and 55.7% against DENV-2. Cases of DENV-3 and DENV-4 weren’t observed.
https://lnkd.in/eAUyiYs8
#dengue #vaccines #Brazil #takeda #sanofi #health #globalhealth #publichealth #medicine #biotechnology #medicine #pharmaceuticals #FDA #CDC #WHO #ECDC #NIAID #clinicaltrials #immunology
|
|
Scooped by
Gilbert C FAURE
March 12, 1:50 PM
|
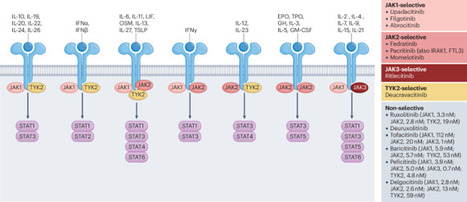
JAK inhibitors target a large group of cytokines that signal through the JAK–STAT pathway and are typically used clinically as immunosuppressive agents. However, recent work has demonstrated the paradoxical ability of JAK inhibitors to enhance antitumour and antiviral immune responses and established their synergy with immune checkpoint inhibitors in early-stage clinical trials. In this Perspective, we consider why JAK inhibitors, which are typically used as immunosuppressive drugs, can have immune-enhancing effects, exploring the potential mechanistic basis and the opportunities to harness this effect to improve cancer immunotherapy. JAK inhibitors are typically used to suppress the immune system but have also been shown to enhance antitumour and antiviral immune responses. In this Perspective, Zak and Teijaro explore the basis of the immune-enhancing properties of JAK inhibitors and consider whether we can exploit these properties for cancer therapy.
|
|
Scooped by
Gilbert C FAURE
March 10, 2:46 PM
|
TWiV 1303: Overachieving vaccines 〰️ TWiV reviews an association between shingles vaccination and slower biological aging, and how mucosal immunization in mice provides protection against disease caused by diverse viruses and bacteria. Hosts: Vincent Racaniello, Alan Dove, Rich Condit, and Brianne Barker. 📺 bit.ly/4lgWW0w
|
|
Scooped by
Gilbert C FAURE
February 25, 3:29 AM
|
𝗔𝗗𝗖𝘀, 𝗮 𝗿𝗲𝘃𝗶𝗲𝘄
🧠 𝗔 𝗽𝗮𝗽𝗲𝗿 𝗮 𝗱𝗮𝘆 𝗸𝗲𝗲𝗽𝘀 𝗯𝗿𝗮𝗶𝗻 𝗱𝗲𝗰𝗮𝘆 𝗮𝘄𝗮𝘆 🧠
Monday, 23 February 2026
𝘈𝘯𝘵𝘪𝘣𝘰𝘥𝘺–𝘥𝘳𝘶𝘨 𝘤𝘰𝘯𝘫𝘶𝘨𝘢𝘵𝘦 𝘱𝘦𝘳𝘧𝘰𝘳𝘮𝘢𝘯𝘤𝘦 𝘪𝘴 𝘳𝘢𝘳𝘦𝘭𝘺 𝘢𝘣𝘰𝘶𝘵 𝘵𝘩𝘦 𝘢𝘯𝘵𝘪𝘣𝘰𝘥𝘺 𝘢𝘭𝘰𝘯𝘦: 𝘭𝘪𝘯𝘬𝘦𝘳 𝘤𝘩𝘦𝘮𝘪𝘴𝘵𝘳𝘺, 𝘱𝘢𝘺𝘭𝘰𝘢𝘥 𝘤𝘭𝘢𝘴𝘴, 𝘢𝘯𝘥 𝘥𝘳𝘶𝘨-𝘵𝘰-𝘢𝘯𝘵𝘪𝘣𝘰𝘥𝘺 𝘳𝘢𝘵𝘪𝘰 𝘥𝘦𝘧𝘪𝘯𝘦 𝘵𝘩𝘦 𝘵𝘩𝘦𝘳𝘢𝘱𝘦𝘶𝘵𝘪𝘤 𝘪𝘯𝘥𝘦𝘹.
💡𝗧𝗮𝗸𝗲 𝗵𝗼𝗺𝗲 𝗺𝗲𝘀𝘀𝗮𝗴𝗲
• Wang et al. detail antibody selection constraints: antigen density/internalization, Fc effector balance, and affinity-driven “binding-site barrier” effects on tumor penetration.
• Linker chemistry defines therapeutic index: cleavable (pH, disulfide, protease, glycosidase) versus non-cleavable designs govern stability and intracellular payload release.
• Payload classes center on tubulin inhibitors and topoisomerase-I poisons; drug-to-antibody ratio control remains a key manufacturability and pharmacology challenge.
🔥𝗜𝗺𝗽𝗮𝗰𝘁
• The review positions linker and payload engineering, alongside drug-to-antibody ratio control, as central levers for next-generation antibody–drug conjugate design.
❓𝗢𝗽𝗲𝗻 𝗾𝘂𝗲𝘀𝘁𝗶𝗼𝗻𝘀
• Can drug-to-antibody ratio heterogeneity be standardized analytically across diverse conjugation chemistries and payload scaffolds?
• Which linker architectures optimize bystander killing while minimizing systemic payload leakage in heterogeneous tumor microenvironments?
• How should Fc effector function be tuned when combining antibody–drug conjugates with immunotherapies to avoid additive toxicity?
𝗔𝗻𝘁𝗶𝗯𝗼𝗱𝘆–𝗗𝗿𝘂𝗴 𝗖𝗼𝗻𝗷𝘂𝗴𝗮𝘁𝗲𝘀 (𝗔𝗗𝗖𝘀): 𝗰𝘂𝗿𝗿𝗲𝗻𝘁 𝗮𝗻𝗱 𝗳𝘂𝘁𝘂𝗿𝗲 𝗯𝗶𝗼𝗽𝗵𝗮𝗿𝗺𝗮𝗰𝗲𝘂𝘁𝗶𝗰𝗮𝗹𝘀
Ruili Wang et al
Journal of Hematology & Oncology, April 2025
Corresponding author(s): Chen Fu, Minjie Wei, Lifeng Yu
🔗 𝘓𝘪𝘯𝘬 𝘵𝘰 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤𝘢𝘵𝘪𝘰𝘯 𝘪𝘯 𝘤𝘰𝘮𝘮𝘦𝘯𝘵𝘴
𝘛𝘩𝘦 𝘰𝘱𝘪𝘯𝘪𝘰𝘯𝘴 𝘴𝘩𝘢𝘳𝘦𝘥 𝘰𝘯 𝘓𝘪𝘯𝘬𝘦𝘥𝘐𝘯 𝘢𝘳𝘦 𝘮𝘺 𝘰𝘸𝘯.
|
|
Scooped by
Gilbert C FAURE
February 19, 3:44 AM
|
Mpox is the topic for this week’s VEC Vaccine Notes episode. Check out this clip for a reminder of when and where monkeypox virus was discovered — and who was the first person diagnosed with mpox.
Find out more about the disease and vaccine in the full episode.
https://lnkd.in/ebQu7f4h
|