NEW YORK—Kidney Disease: Improving Global Outcomes (KDIGO) today released a new Clinical Practice Guideline for Anemia in Chronic Kidney Disease (CKD).
The interim futility analysis for cema-cel, just gave the lymphoma field something to think about. A 41.6% absolute difference in MRD negativity at Day 45 versus observation, with clean tolerability, availability in community hospitals and most patients managed as outpatients. It is a meaningful signal that allogeneic CAR-T can work in first-line consolidation post R-CHOP.
What about the patients who relapse after cema-cel? Go back to CD19 with an autologous product: Yescarta, Breyanzi? They all target the same CD19 as cema-cel. Would a second CD19 CAR-T be reimbursed? If cema-cel moves towards commercialization in LBCL, patients who relapse will need a subsequent differentiated option. The commercial case for CD19-targeted autologous therapies in this setting will need rethinking.
This is where eti-cel becomes relevant. A highly differentiated product also developed at Cellectis, on the same backbone as cema-cel (originated from Cellectis platform), eti-cel targets both CD20×CD22 simultaneously. Data at the current dose show 88% ORR and 63% CR in heavily pretreated patients, a strong signal for a dual allogeneic approach.
Fifteen years ago, CAR-T emerged as a revolution. The real breakthrough, the bona fide pharmaceutical product, is allogeneic. Off-the-shelf, scalable, standardized. It will establish a new order in cell therapy. Autologous therapies are a process and will, in time, disappear.
On in vivo CAR-T: the science is early, the toxicity profile remains unfavorable today, and the regulatory path for a therapy where the vector is the product is, at best, unclear.
Cellectis Allogene Therapeutics Kite Pharma Bristol Myers Squibb Novartis Johnson & Johnson Gilead Sciences #dlcl #CART #celltherapy #allogeneic | 14 comments on LinkedIn
On behalf of the International Society for Laboratory Hematology (ISLH), we cordially invite you to attend the International Symposium on Technological Innovations in Laboratory Hematology.
The College is pleased to have endorsed the British Society for Haematology report “The Haematology Workforce: A Comprehensive View.”
This report highlights the vital role of clinical pathology and laboratory services in the rapid diagnosis and management of haematological diseases.
The report reveals the growing pressure on haematology professionals, as the gap between workforce capacity and clinical demand continues to widen.
Supporting these findings, the College’s 2025 Workforce Census finds that 82% of haematologists believe current staffing levels are insufficient to ensure the long-term sustainability of services.
The College agrees that robust workforce planning is essential to align haematology services with local and regional needs – factoring in population growth, diagnostic demand, evolving working patterns, and succession planning.
Action and investment are urgently needed to future-proof the haematology workforce and ensure equitable access to high-quality care for all affected by blood diseases.
Hemophagocytic lymphohistiocytosis (HLH) is a severe and life-threatening syndrome characterized by overwhelming inflammation that often leads to multiorgan…
#EpsteinBarrVirus hijacks #Bcell #Metabolism to establish persistent infection and drive #Pathogenesis | Open Access Review by Bojana Müller et al breaking at…
ASH Annual Meeting Abstracts Latest Announcements Late-Breaking Abstracts Now Available Late-breaking abstracts feature substantive, novel, and groundbreaking data that were not available by the general abstract submission deadline and would otherwise not be presented at the ASH annual meeting. View the 2024 Late-Breaking Abstracts 2024 ASH Annual Meeting Abstracts Abstracts for the 2024 ASH Annual Meeting and Exposition, including late-breaking abstracts, are now available. A record-breaking number of abstracts were submitted and more than 7,950 were accepted. View the accepted abstracts representing the most cutting-edge science in hematology. View the 2024 Abstracts About ASH Annual Meeting Abstracts Abstracts submitted for oral and poster presentation at the ASH annual meeting represent important, novel research in the field and are considered the best of the thousands of abstracts submitted. Typically, more than 7,000 scientific abstracts are submitted each year, and more than 5,000 abstracts are accepted for oral and poster presentations through an extensive peer review process. Abstract categories are reviewed and updated annually to respond to trends and cover new areas. This year, updates include The renumbering of categories (particularly those in the 600 and 900 groupings) The discontinuation of two categories (731. Autologous Transplantation, and 705. Cellular Immunotherapies: Commercial and Late Stage) The addition of several new categories (909. Education, Communication, and Workforce, 628. Aggressive Lymphomas: Cellular Therapies, and 655. Multiple Myeloma: Cellular therapies) The splitting of several categories (including several in thrombosis and homeostasis, clinical lymphomas, and health services, quality improvement and outcomes research). View the full list of abstract categories. The Plenary Scientific Session, which includes the top six abstracts as selected by the Program Committee, is traditionally a highlight of the annual meeting program. View the 2024 Abstracts Key Dates and Deadlines Abstract submission site opens May 30, 2024 Abstract submission deadline August 1, 2024, 11:59 p.m. Pacific time Abstract withdrawal deadline September 18, 2024 Call for late-breaking abstract submissions October 16-28, 2024 Abstracts available online November 5, 2024, 9:00 a.m. Eastern time Abstract poster presentation materials due November 12, 2024 Late-breaking abstracts available online November 25, 2024, 9:00 a.m. Eastern time Related Content Call for Late-Breaking Abstracts Late-breaking abstract submissions for the 2024 ASH Annual Meeting and Exposition are open from October 16, 2024, through October 28, 2024, at 11:59 p.m. Pacific time. No submissions will be accepted after this deadline. Learn More > Call for Abstracts Abstract submissions for the 2024 ASH Annual Meeting and Exposition are open from May 30, 2024, through August 1, 2024, at 11:59 p.m. Pacific time. No submissions will be accepted after this deadline. Learn More > Poster Walks Poster Walks highlight abstracts submitted to the annual meeting that showcase emerging science in hematology. Learn More > Copyright and Reuse Policy Material presented at the annual meeting is subject to copyright or other reuse restrictions. Learn More > Abstract Achievement Awards Merit-based awards are provided to trainees with high-scoring annual meeting abstracts of which they are the first or senior author and presenter. Learn More > 66th ASH Annual Meeting and exposition Registration for ASH members, non-members, groups, exhibitors, and media is now open! View Additional Information Explore the Annual Meeting Schedule and Program Hotel and Travel Information Abstracts Meeting and Presenter Resources CME and MOC Information Code of Conduct
Using video microscopy in the living mouse lung, UC San Francisco scientists have revealed that the lungs play a previously unrecognized role in blood production.
Immune cells continually detect, engulf, and destroy invasive microbes and cancer cells.
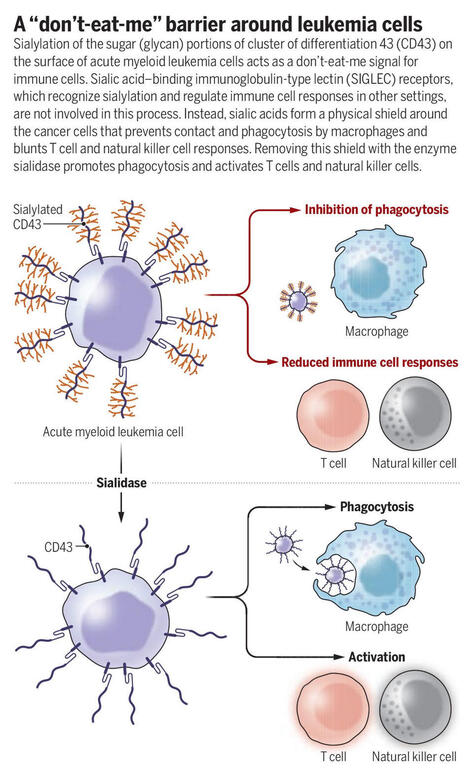
This process, called phagocytosis, is carried out by macrophages that must distinguish between proengulfment signals and inhibitory (“don’t-eat-me”) warnings. Cluster of differentiation 47 (CD47), a cell-surface receptor, is the archetypal don’t-eat-me signal. Many cancers upregulate CD47 expression to escape phagocytosis, and CD47 blockade promotes phagocytosis of cancer cells in mice.
However, CD47 blockers have not shown clinical benefits in patients with acute myeloid leukemia (AML), an aggressive cancer of blood immune cells. This discrepancy has raised the possibility that the molecular programs that inhibit phagocytosis differ between mice and humans.
In a new Science study, researchers report that the mechanisms that control macrophage function in human and mouse cells are indeed different. They also identify cluster of differentiation 43 (CD43) as a potential target for human AML treatment.
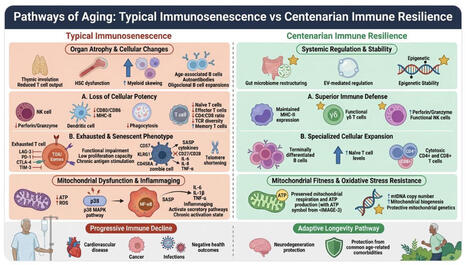
𝗜𝗺𝗺𝘂𝗻𝗼𝘀𝗲𝗻𝗲𝘀𝗰𝗲𝗻𝗰𝗲 is a multimodal immune system remodeling process that includes inflammation, cellular senescence, T-cell fatigue, and thymic involution, all of which raise the risk of infection and disease as we age. Our review published in Current Opinion in Immunology https://lnkd.in/efRp3D4M highlights that centenarians often exhibit adaptive remodeling and maintained immune balance rather than a uniform decline. This includes retention of naïve T cells, expansion of cytotoxic T cell subsets, and regulated inflammatory signaling.
➡️ Immunosenescence should be viewed as a trajectory-dependent process in which balanced immune function determines resilience and healthy aging.
➡️ Progress in understanding immunosenescence is dependent on integrating longitudinal multi-omics data to generate biological-age biomarkers and inform immunometabolic or senotherapeutic techniques for extending healthspan. Thanks to coauthors Ivan David Lozada Martinez, MD, MSc Yeny Acosta Ampudia Gabriel Tobón
Every second, your body creates 2 million brand new red blood cells. Did you know they all die in exactly 120 days and your spleen processes 200 billion dead cells daily? Follow for more mind-blowing health facts! #health #bloodcells #humanbody #biology #shorts
Peter Voorhees, MD, emphasizes the importance of carefully determined early regimens for smoldering myeloma and involving patients in treatment decisions.
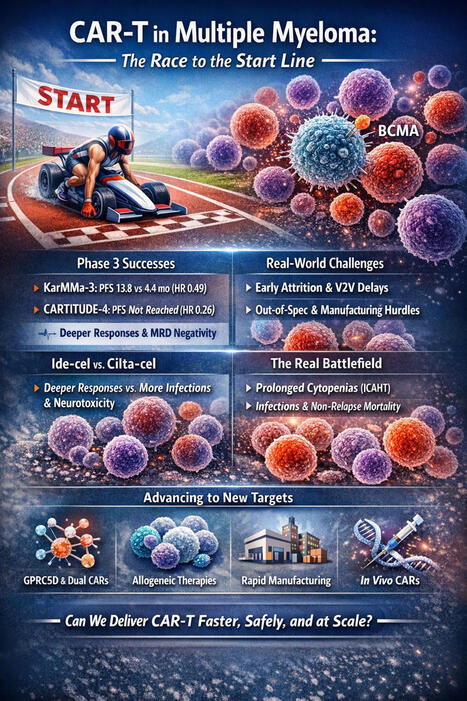
🧬🏁 CAR-T in Multiple Myeloma is no longer just a response-rate story — it’s a race to the “start line.” BCMA CAR-T has reset expectations in relapsed/refractory MM… and now the field is pushing earlier. But this review makes one point crystal clear: randomized medians don’t tell you who actually reaches infusion or who survives the logistics. s41409-025-02787-9 🔥 What the phase 3 data proved (earlier lines) 📌 KarMMa-3: ide-cel beat standard regimens with PFS 13.8 vs 4.4 months (HR 0.49), deeper responses, and higher MRD negativity. 📌 CARTITUDE-4: cilta-cel delivered even stronger separation: PFS not reached vs 11.8 months (HR 0.26), plus improved MRD and an OS advantage in later analysis (HR 0.55). s41409-025-02787-9 ⚠️ What trials don’t capture (and practice can’t ignore) ⏳ Attrition before infusion is real early deaths often occur in patients who never receive CAR-T while waiting through bridging + manufacturing windows. 🏭 Vein-to-vein (V2V) and “brain-to-vein” delays shape outcomes as much as biology. 🧪 Out-of-spec (OOS) products and manufacturing variability are not edge cases in the real world. s41409-025-02787-9 🧠 Product-specific reality: ide-cel vs cilta-cel ✅ The review highlights a consistent signal: cilta-cel tends to deliver deeper and more durable responses, but with more infections and distinct delayed neurotoxicity patterns that require long-horizon vigilance. s41409-025-02787-9 🛡️ The real battlefield: cytopenias + infections After the acute CRS/ICANS window, the dominant risks become: 🩸 prolonged cytopenias (ICAHT) + 🦠 infections, driving non-relapse mortality in routine care and strongly influenced by bridging intensity and baseline inflammatory/hematologic risk tools (e.g., CAR-HEMATOTOX; albumin+CRP). s41409-025-02787-9 🚀 What could move the start line forward 🎯 Beyond-BCMA targets (GPRC5D) 🧬 dual/multi-antigen CARs to curb escape (especially in EMD / post-BCMA) 🏭 next-day / point-of-care manufacturing 🧊 allogeneic off-the-shelf strategies 🧫 even in vivo CAR concepts designed to bypass apheresis and ex vivo manufacturing s41409-025-02787-9 💬 If CAR-T is moving earlier, the key question isn’t only “Can it beat SOC?” it’s “Can we deliver it fast, safely, and at scale?” #MultipleMyeloma #CarT #CiltaCel #IdeCel #CellTherapy #Immunotherapy #Hematology #Oncology #BCMA #GPRC5D
Over the past decades, the progressive identification of chromosomal abnormalities and gene mutations has transformed acute myeloid leukemia (AML) fro…
0:00 Introduction 0:45 What Is Systems-Based Hematology? 1:30 Gaps in the Field 2:05 ASH Study and Results 6:40 Designing a Curriculum 8:56 How This Affects Patients
In this episode, Dr. Richard Godby shares more about his team’s ASH presentation on creating a standardized curriculum for systems-based hematology, including gaps, challenges, and future directions in this emerging discipline.
Learn about: - What systems-based hematology means - His team’s study interviewing experts in the field - Themes that the interviews revealed - How these results can be used to inform the development of educational resources and training programs for systems-based hematology - Next steps for the research - How this research might affect patient care - And more!
📝Publié ! 6 ans après le début de ce projet qui s’inscrit dans la continuité de la recherche de l’équipe du Pr Eric Solary à Gustave Roussy, les résultats de…
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.






 Your new post is loading...
Your new post is loading...