Your new post is loading...
Your new post is loading...

|
Scooped by
Gilbert C FAURE
February 21, 2022 3:32 AM
|
|
|
Scooped by
Gilbert C FAURE
February 18, 2022 6:00 AM
|
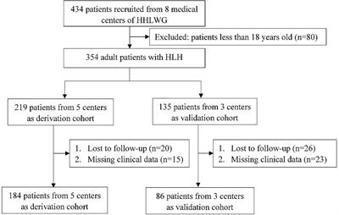
Hemophagocytic lymphohistiocytosis (HLH) is an immune disorder with rapid progression and poor survival. Individual treatment strategy is restricted, due to the absence of precise stratification criteria. In this multicenter retrospective study, we aimed to develop a feasible prognostic model for adult HLH in China. A total of 270 newly diagnosed patients of adult HLH were retrieved from the Huaihai Lymphoma Working Group (HHLWG), of whom 184 from 5 medical centers served as derivation cohort, and 86 cases from 3 other centers served as validation cohort. X-Tile program and Maxstat analysis were used to identify optimal cutoff points of continuous variables; univariate and multivariate Cox analyses were used for variable selection, and the Kaplan–Meier curve was used to analyze the value of variables on prognosis. The C-index, Brier Score, and calibration curve were used for model validation. Multivariate analysis showed that age, creatinine, albumin, platelet, lymphocyte ratio, and alanine aminotransferase were independent prognostic factors. By rounding up the hazard ratios from 6 significant variables, a maximum of 9 points was assigned. The final scoring model of HHLWG-HPI was identified with four risk groups: low risk (≤3 pts), low-intermediate risk (4 pts), high-intermediate risk (5-6 pts), and high risk (≥7 pts), with 5-year overall survival rates of 68.5%, 35.2%, 21.3%, and 10.8%, respectively. The C-indexes were 0.796 and 0.758 in the derivation and validatio
|
|
Scooped by
Gilbert C FAURE
February 6, 2022 1:57 PM
|
COVID-19 significantly impairs survival rates among hematological patients when compared to the general population.Our prospective multicentre project analyzed early administration of anti-SARS-CoV-2 spike protein neutralizing monoclonal antibodies (NmAbs) - bamlanivimab (72%) and casirivimab / imd...
|
|
Scooped by
Gilbert C FAURE
January 26, 2022 8:27 AM
|
“These studies are the result of tremendous efforts by our colleagues in the United States and Iceland. Identifying and intervening with therapy for patients with monoclonal gammopathy at high risk for disease progression and end-organ damage may become standard in the near future,” said Dr.
|
|
Scooped by
Gilbert C FAURE
December 31, 2021 11:10 AM
|
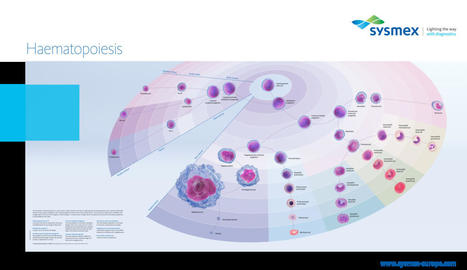
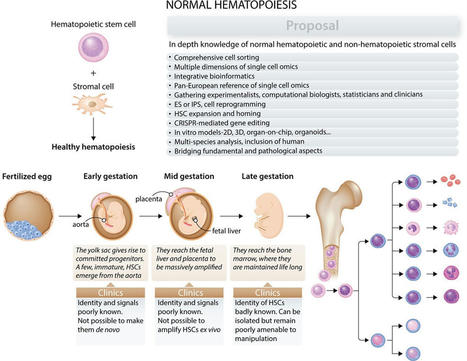
An interactive illustration of blood cell development, an introduction to haematopoiesis and the role haematology analysers play.
|
|
Scooped by
Gilbert C FAURE
December 29, 2021 3:06 AM
|
Kikuchi-Fujimoto disease (KFD) is a reactive lymphadenitis of unclear etiology. To understand the pathogenesis of KFD, we performed targeted RNA sequencing of a well-characterized cohort of 15 KFD specimens with 9 non-KFD lymphadenitis controls. Two thousand and three autoimmunity-related genes were evaluated from archived formalin-fixed paraffin-embedded lymph node tissue and analyzed by a bioinformatics approach. Differential expression analysis of KFD cases compared to controls revealed 44 significantly upregulated genes in KFD. Sixty-eight percent of these genes were associated with the type I interferon (IFN) response pathway. Key component of the pathway including nucleic acid sensors, IFN regulatory factors, IFN-induced antiviral proteins, IFN transcription factors, IFN-stimulated genes, and IFN-induced cytokines were significantly upregulated. Unbiased gene expression pathway analysis revealed enrichment of IFN signaling and antiviral pathways in KFD. Protein–protein interaction analysis and a molecular complex detection algorithm identified a densely interacting 15-gene module of type I IFN pathway genes. Apoptosis regulator IFI6 was identified as a key seed gene. Transcription factor target analysis identified enrichment of IFN-response elements and IFN-response factors. T-cell-associated genes were upregulated while myeloid and B-cell-associated genes were downregulated in KFD. CD123+ plasmacytoid dendritic cells (PDCs) and activated T cells were noted in KFD. In conclusion, KFD is mediated by an aberrant type I interferon response that is likely driven by PDCs and T cells.
|
|
Scooped by
Gilbert C FAURE
December 13, 2021 1:12 PM
|
6,365 ALL-related posts were identified; 289 (4.5%) were contributed by patients, 657 (10.3%) by CGs, 1224 (19.2%) by HCPS and 4,195 (65.9%) by organizations. Topics included expressions of positive support/encouragement for patients/monetary donation requests/treatment type/impact of side effects. NLU identified notable discussion areas: patient/CG commentaries on treatment experiences, decisions, side effects and outcomes, and patient knowledge regarding ALL treatments. 189 patient/CG posts discussed ALL treatments in general, including in-hospital time: missing life events due to intensive treatment regimens and extended hospital stays. 195 patient/CG posts discussed specific ALL treatment experiences: chemotherapy, n=120; bone marrow transplant, n=22; stem cell transplant, n=16; immunotherapy, n=14; Kymriah, n=11; CAR-T, n=8; radiation, n=4. Chemotherapy was mentioned in relation to daily and/or durable short-and long-term effects (e.g., sickness, pain) which had major impacts for patients’ and their family’s HRQOL. Chemotherapy was associated with unforeseen impacts related to patients compromised immune systems (e.g., restricted social functioning due to increased risk of infection). Fear of infection and impact of treatment notably increased patients’ needs to isolate which had a substantial impact on the broader family life. Bone marrow transplant posts described it as ‘lifesaving’. Despite uncertainty of treatment success and negative treatment effects, patient/CG posts noted that side effects were an acceptable part of the journey to become cancer free. Posts also illustrated a general shift in patient/CG perception of ALL treatments, specifically that no one treatment works for everyone in the same way, and recent treatment developments mean that ALL is no longer perceived as a death sentence. 66 patient/CG posts commented on the cessation of treatment or lack of treatment due to remission, alternative treatments or end of life. Financial burden due to ALL treatment was an important issue for patients/CGs as it prevented the start of treatment or impaired patients’/CGs’ lives.
|
|
Scooped by
Gilbert C FAURE
November 29, 2021 3:32 AM
|
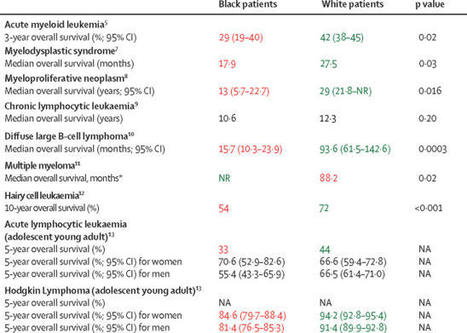
Most studies of racial and ethnic survival disparities in patients with cancer diagnosed
and treated in the USA have pertained to patients with solid tumours. However, increasing
research on health inequities shows that these differences also extend to patients
with haematological malignancies.
|
|
Scooped by
Gilbert C FAURE
November 28, 2021 6:45 AM
|
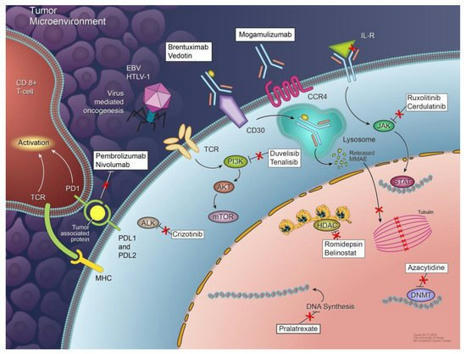
T-cell lymphomas are a relatively rare group of malignancies with a diverse range of pathologic features and clinical behaviors. Recent molecular studies have revealed a wide array of different mechanisms that drive the development of these malignancies and may be associated with resistance to...
|
|
Scooped by
Gilbert C FAURE
November 8, 2021 9:19 AM
|
Bruton tyrosine kinase (BTK) inhibitors represent an important therapeutic advancement for B cell malignancies. Ibrutinib, the first-in-class BTK inhibitor, is approved by the US FDA to treat patients with chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL), and mantle cell...
|
|
Scooped by
Gilbert C FAURE
October 13, 2021 11:31 AM
|
Live-Webinar October 12, 2021: Dr Balyn Zaro of University of California: "Proteomic analysis of adult and aged mouse hematopoietic stem cells and their progenitors"...
|
|
Scooped by
Gilbert C FAURE
October 6, 2021 5:03 AM
|
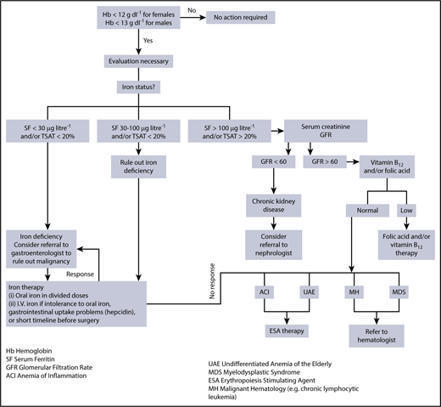
Abstract.Anemia of inflammation (AI), also known as anemia of chronic disease (ACD), is regarded as the most frequent anemia in hospitalized and chronically il...
|
|
Scooped by
Gilbert C FAURE
September 2, 2021 8:36 AM
|
Iron-Deficiency Anemia IDA is classically a microcytic and hypochromic anemia, reflected as a decreased MCV and mean corpuscular Hb concentration (MCHC), respectively. From: Hematopathology (Second Edition), 2012 Related terms: FerritinIron Storage View all Topics Iron Deficiency Anemia In Diagnostic Pathology: Blood and Bone Marrow (Second Edition), 2018 Clinical Issues • Iron deficiency anemia is most common anemia worldwide; estimated global anemia prevalence is 24.8%, affecting > 1.62 billion people • Insidious onset, chronic, often asymptomatic • Symptoms may include fatigue, pallor, weakness, tachycardia, dyspnea on exertion • Diagnosis of iron deficiency anemia should be based on panel of tests, not on any single test • Low serum ferritin is pathognomonic of iron deficiency anemia • Serum transferrin saturation < 16% supports diagnosis of iron deficiency • Oral ferrous iron salt (ferrous sulfate) supplementation to all patients with iron deficiency • Parenteral iron should be given to patients who cannot take or are refractory to oral iron supplement • Red blood cell transfusion should be given to patients with symptomatic severe iron deficiency anemia to rapidly correct hypoxia and iron deficiency • Excellent prognosis except in patients with underlying disease Hematology and hemostasis in the pediatric, geriatric, and pregnant populations Linda H. Goossen, in Rodak's Hematology (Sixth Edition), 2020 Iron deficiency anemia. Iron deficiency anemia is the most common pediatric hematologic disorder and the most common cause of anemia in childhood.22,23 Iron deficiency anemia is more prevalent in premature infant because the majority of the placental transfer of maternal iron occurs late in the third trimester.4 The occurrence of iron deficiency anemia in infants has decreased in the United States because of iron fortification of infant formula and increased rates of breastfeeding.24 However, the prevalence is still 2% in toddlers 1 to 2 years of age and 3% in children 3 to 5 years of age25 and is related to early introduction and excessive intake of whole cow’s milk.20,25 Chapter 17 provides an in-depth discussion of iron deficiency anemia. Circulatory, Reticuloendothelial, and Hematopoietic Disorders Anne L. Grauer, in Ortner's Identification of Pathological Conditions in Human Skeletal Remains (Third Edition), 2019 Iron-Deficiency Anemia IDA, or acquired anemia, is the most common type of anemia found globally. It is associated with the presence of microcytic and hypochromic RBC, along with depressed levels of total body iron (Camaschella, 2015). Bone changes in IDA tend to be clinically mild. Changes in the skull vault resemble those described for other anemias, i.e., radiographically recognizable enlargement of the diploë with vertical orientation of the trabeculae. Aksoy et al. (1966) report that generalized granular osteoporosis of the skull and long bones might also appear in some patients. IDA has received the greatest attention as a diagnostic option for porous hypertrophic lesions of the skull in the paleopathological record. However, the tendency for this anemia to produce only limited skeletal involvement has raised questions about the legitimacy of the diagnosis. Importantly, a wide range of conditions invoke an anemic response by the body, rendering the isolation of the cause of hypertrophic lesions extremely difficult (Table 14.2). Table 14.2. Causes of Iron Deficiency and Iron-Deficiency Anemia Environmental Insufficient dietary intake Dietary restrictions or predilection (grain intensive, vegetarian, vegan, etc.) Genetic Iron-refractory iron-deficiency anemia Pathologic Decreased absorption Atrophic gastritis Celiac sprue Helicobacter pylori infection Inflammatory bowel diseases Parasitic infestation Chronic blood loss Gastrointestinal tract Benign and malignant tumors Diverticulitis Erosive gastritis Esophagitis Hookworm infestation Peptic ulcer Genitourinary system Intravascular hemolysis Heavy mensis or menorrhagia Systemic bleeding Chronic schistosomiasis Hemorrhagic telangiectasia Physiologic Increased demand for iron Infancy Rapid growth (adolescence) Menstruation Pregnancy Source: After Camaschella (2015). Pediatric Transfusion in Developing Countries Kenneth A. Clark MD, MPH, in Handbook of Pediatric Transfusion Medicine, 2004 Nutritional Anemia Iron deficiency anemia is highly prevalent in many developing countries. The WHO estimates that as many as 50% of children in developing countries have iron-deficiency anemia (WHO 2001). Rural populations with more restricted resources and lower educational levels may be more severely affected than urban populations. Infants who have been breast-fed for more than 4 to 6 months are particularly susceptible if their diets are not supplemented with foods rich in iron or dietary supplements. In some areas, the use of iron supplements is limited by resources. Inadequate dietary intake of vitamin B12 or folate also contributes to pediatric anemia. Dietary insufficiencies are often compounded by additional illnesses such as diarrheal diseases that further impair intestinal absorption. Disorders of Red Blood Cells James W. Little DMD, MS, ... Nelson L. Rhodus DMD, MPH, in Little and Falace's Dental Management of the Medically Compromised Patient (Eighth Edition), 2013 Iron Deficiency Anemia Iron deficiency anemia is a microcytic anemia (Figure 22-2) that can be caused by excessive blood loss, poor iron intake, poor iron absorption, or increased demand for iron. Blood loss may occur with menstruation or be caused by bleeding from the gastrointestinal tract. Poor intake is more common in children who live in developing countries, where cereals and formula fortified with iron are not readily available. Malabsorption of iron can result from gastrectomy or intestinal disease that reduces absorption of iron from the duodenum and the jejunum. Increased demand is associated with chronic inflammation (autoimmune disease). In women, menstruation and pregnancy contribute to the development of iron deficiency anemia. The repeated loss of blood associated with menses can lead to depletion of iron, resulting in a mild state of anemia. During pregnancy, the expectant mother experiences an increased demand for additional iron and vitamins to support the growth of her fetus, and unless sufficient amounts of these nutrients have been provided in some form, she may become anemic. Approximately 20% of pregnant women have iron deficiency anemia.11 Also, 30% to 60% of persons with rheumatoid arthritis (who more commonly are women) have this type of anemia.12 By contrast, mild anemia in men usually indicates the presence of a serious underlying medical problem (e.g., gastrointestinal bleeding, malignancy). Under normal physiologic conditions, men lose little iron, and because iron can be stored for months, iron deficiency anemia is rare in men. Therefore, any man who is found to be anemic should be promptly referred for medical evaluation. Red-Blue Lesions In Oral Pathology (Sixth Edition), 2012 Iron Deficiency Anemia Etiology Iron deficiency anemia is a rather common anemia caused by iron deficiency. This deficiency may be due to inadequate dietary intake; impaired absorption caused by a gastrointestinal malady; chronic blood loss caused by such problems as excessive menstrual flow, gastrointestinal bleeding, or aspirin ingestion; and increased demand as experienced during childhood and pregnancy. Clinical Features This relatively prevalent form of anemia predominantly affects women. In addition to the clinical signs and symptoms associated with anemias in general, iron deficiency anemia may result in brittle nails and hair and koilonychia (spoon-shaped nails). The tongue may become red, painful, and smooth. Angular cheilitis may also be seen. In addition to iron deficiency, the Plummer-Vinson (Paterson-Kelly) syndrome includes dysphagia, atrophy of the upper alimentary tract, and a predisposition to the development of oral cancer. Diagnosis Laboratory blood studies show slightly to moderately reduced hematocrit and reduced hemoglobin level. The RBCs are microcytic and hypochromic. The serum iron level is also low, but the total iron-binding capacity (TIBC) is elevated. Treatment Recognition of the underlying cause of iron deficiency anemia is necessary to treat this condition effectively. Dietary iron supplements are required to elevate hemoglobin levels and replenish iron stores once an underlying cause has been defined and treated. Sports Medicine and Adaptive Sports Christopher W. Mcmullen, ... Mark A. Harrast, in Braddom's Physical Medicine and Rehabilitation (Sixth Edition), 2021 Anemia The three most common causes of anemia in the athlete are iron deficiency anemia (IDA), physiologic anemia (pseudoanemia), and foot-strike hemolysis. IDA is most common in menstruating women, and female athletes can be more prone to developing it. The etiology is either blood loss or poor iron intake. Many athletes consume restrictive diets that can have too little iron to meet daily needs. However, a complete history and physical examination are still important to evaluate for “nonathletic” causes such as significant gastrointestinal or genitourinary blood losses. Usually a serologic work-up is diagnostic and includes complete blood count (CBC), serum ferritin, and total iron binding capacity (TIBC). The CBC will show a microcytic anemia.130 Serum ferritin levels that are less than 30 ng/mL in athletes are considered suggestive of IDA.74 The TIBC will be elevated. If IDA is diagnosed, a trial of oral iron supplementation (typically ferrous sulfate or ferrous gluconate, 325 mg three times daily) is undertaken.45 Iron is best absorbed in an acidic environment, so it is concomitantly administered with vitamin C, usually for a 2- to 3-month course. Physiologic anemia is considered a pseudoanemia seen commonly in endurance athletes. Endurance athletes tend to have a lower hemoglobin concentration than the general population because of plasma volume expansion with a dilutional effect. It is an adaptation to exercise and is not considered to inhibit athletic performance. It generally normalizes with training cessation of 3 to 5 days. If IDA is ruled out, there is no necessary treatment. Foot-strike hemolysis refers to red blood cell destruction in the feet from running impact. However, intravascular hemolysis is seen in swimmers, cyclists, and runners, but whether or not actual mechanical red blood cell trauma is the source is questionable. Possible reasons are intramuscular destruction, osmotic stress, and membrane lipid peroxidation caused by free radicals released by activated leukocytes. Intravascular hemolysis can even be regarded as a physiologic means to provide heme and proteins for muscle growth in athletes.213 In general, the hemolysis is mild, and treatment is rarely required. Volume 2 Gerard E. Mullin MD, in Textbook of Natural Medicine (Fifth Edition), 2020 Iron Iron deficiency anemia is very common in IBD, largely because of chronic blood loss through the gut.60 Serum ferritin levels are the most useful indices of iron status. A serum ferritin concentration of greater than 55 ng/mL indicates adequate iron reserves in bone marrow, whereas a concentration of less than 18 ng/mL is highly predictive of iron deficiency (see Chapter 23 for further discussion). The clinician should attempt to increase the patient’s iron stores by improving absorption, as with supplemental vitamin C, rather than through direct iron supplementation, which promotes intestinal infection.71 Red Blood Cell/Hemoglobin Disorders Steven H. Kroft MD, Sara A. Monaghan MD, in Hematopathology (Second Edition), 2012 Clinical Features IDA ranges from mild to profound, with Hb levels as low as 2 g/dL in the most severe cases. IDA is classically a microcytic and hypochromic anemia, reflected as a decreased MCV and mean corpuscular Hb concentration (MCHC), respectively. However, the MCV may be normal in early iron deficiency; the degree of microcytosis roughly correlates with the degree of anemia. Likewise, the MCHC may be normal in early iron deficiency when only a minority of cells are hypochromic. Iron Deficiency Anemia—Fact Sheet Definition ▪ Anemia owing to inadequate iron supply Incidence and Location ▪ Most common cause of anemia worldwide Morbidity and Mortality ▪ Reduced quality of life and reduced productivity ▪ Probably increased maternal and fetal–neonatal morbidity and mortality ▪ Probably reduced cognitive development in children Gender, Race, and Age Distribution ▪ Increased incidence in infants, children, women of childbearing age, and impoverished populations, particularly in underdeveloped countries ▪ Increased incidence in some minorities compared with white population in the United States Clinical Features ▪ General signs and symptoms of chronic anemia ▪ Angular cheilitis, glossitis, pica, koilonychia, and esophageal webs Prognosis and Therapy ▪ Oral iron supplementation ▪ Parenteral iron in patients with uncontrolled blood loss, intolerance to oral iron, or intestinal malabsorption Most signs and symptoms are those seen in any form of anemia, such as fatigue, dyspnea, and pallor of skin and mucous membranes. Because the anemia develops over a protracted period and compensatory mechanisms have ample time to develop, anemia resulting from iron deficiency is surprisingly well tolerated, even when extremely severe. Pica, koilonychia (i.e., spoon-shaped nails), and esophageal webs are rare but have a strong association with IDA. Angular cheilitis and atrophic glossitis are also seen with IDA but are not specific. Pathologic Features The characteristic findings on the peripheral blood film are small (microcytic), underhemoglobinized (hypochromic) RBCs with variability in size (anisocytosis) and abnormal shapes (poikilocytosis; Figure 1-10). Elliptocytes are prominent poikilocytes in IDA; often they are long and narrow (pencil cells). Prekeratocytes are usually evident and are recognized as red cells with sharp-edged, submembranous vacuoles and preserved central pallor (see Figure 1-10). Target cells, teardrop cells, very small hypochromic microcytes, and various nonspecific poikilocytes are also common. Occasional red cell fragments may be observed, but they are not prominent. Thrombocytosis is common, but platelet counts may also be normal or reduced. Variations from the typical findings occur when there has been recent partial repletion of iron or when additional factors, such as Cbl or folate deficiency, are also contributing to anemia. Iron Deficiency Anemia—Pathologic Features Peripheral Blood ▪ Hypochromic, microcytic red blood cells ▪ Anisocytosis ▪ Lack of polychromasia ▪ Poikilocytosis, including elliptocytes, prekeratocytes, and target cells Bone Marrow ▪ Mild erythroid hyperplasia ▪ Absent stainable iron on a Prussian blue stain on an aspirate smear Differential Diagnosis ▪ Thalassemia trait or thalassemia-like hemoglobinopathy ▪ Anemia of chronic disease The bone marrow in IDA may demonstrate erythroid hyperplasia, but this is generally of only a mild degree. Erythroid precursors may have scant cytoplasm with frayed cytoplasmic borders. Ancillary Studies Serum ferritin measurement is the most useful single laboratory test for iron deficiency. Serum ferritin below the lower limit of the reference range (about 12 mg/dL) is essentially diagnostic of iron deficiency. However, ferritin is an acute-phase reactant, and normal levels may be seen when iron deficiency coexists with infection, inflammation, or malignancy. However, when this occurs, the ferritin level will usually be low-normal; therefore low-normal values in an individual with an active inflammatory process support a diagnosis of iron deficiency in the appropriate setting. Ferritin levels may even be higher in patients with acute liver injury, despite iron deficiency. Measurement of serum iron alone is not useful because of diurnal fluctuations of serum iron levels and the rapid changes that may occur with dietary intake, inflammation, and blood loss. Transferrin, measured either directly or indirectly as the total iron binding capacity, is typically increased in IDA, but this response can be blunted in the presence of hypoproteinemia. The transferrin saturation (the ratio of serum iron to total iron binding capacity) is typically less than 15% in iron deficiency, but saturation levels in this range may also be seen in ACD. Increased serum soluble transferrin receptor (sTfR) is a sensitive marker of iron deficiency, reflecting increased expression of this receptor on RBC precursors as a response to depleted tissue iron. This parameter is elevated during iron-deficient erythropoiesis before the development of overt anemia. Furthermore, inflammation does not raise sTfR levels substantially. However, states with an increased mass of RBC precursors such as hemolytic anemias and ineffective erythropoiesis (e.g., megaloblastic anemia) will manifest elevated sTfR; therefore this finding is not specific for iron deficiency. When biochemical tests are equivocal, the absence of stainable iron with a Prussian blue stain performed on well-prepared marrow aspirate smear is considered to be the gold standard for the diagnosis of IDA. An iron stain performed on a bone marrow core biopsy may also be helpful, but iron can be leached out during decalcification of the bone marrow biopsy and result in the false interpretation of absent iron stores. Differential Diagnosis Other common causes of hypochromic, microcytic anemia are thalassemia and ACD. Sideroblastic anemia with microcytosis is rarer. The hematologic and biochemical tests that are useful to differentiate the major causes of microcytic anemia are listed in Table 1-3. In addition, mild anemia associated with thalassemia trait or a thalassemia-like hemoglobinopathy (e.g., Hb E) characteristically exhibits a red blood cell count greater than 5 × 1012 cells/L, which is unusual for IDA. Hb electrophoresis would help establish the diagnosis of most β-thalassemias and thalassemia-like hemoglobinopathies. Under circumstances that render the interpretation of biochemical studies for iron status particularly difficult, such as inflammation, monitoring the response of Hb or the reticulocyte count to a therapeutic trial of iron supplementation may be sufficient to confirm iron deficiency. Otherwise, any uncertainty about iron status usually can be resolved by an iron stain performed on a bone marrow aspirate smear. Pathological Conditions Efthymia Nikita, in Osteoarchaeology, 2017 8.5.4 Iron-Deficiency Anemia Iron-deficiency anemia results from reduced iron availability in the red blood cells (Box 8.5.3). Iron is an integral component of the hemoglobin molecule and its main function is the transport of oxygen to various bodily tissues. Iron-deficient red blood cells are generally small (microcytic), are pale (hypochromic), have a short life span, and are incapable of transporting oxygen efficiently (Kozłowski and Witas, 2011). The factors that may reduce iron availability include malnutrition, parasitic infestations that inhibit iron absorption, infection that makes the body withhold iron, profuse hemorrhage, or increased iron demands during growth or pregnancy (Holland & O'Brian, 1997; Stuart-Macadam, 1989; Sullivan, 2005). Box 8.5.3 Skeletal Manifestations of Iron-Deficiency Anemia (Stuart-Macadam, 1992; Sullivan, 2005) • Skull • Enlarged diploë, thinned cortical bone layer, thickened vault (PH) • Porosity of the orbital roof (CO) • Long bones • Osteoporosis With regard to diet, heme iron is found primarily in meat and it is easily absorbed through the intestine, whereas nonheme iron may be obtained through consumption of cereals, legumes, fruits, and vegetables but it is less bioavailable. Moreover, phytates, tannins, and other food compounds can bind iron into complex formations that cannot be absorbed by the intestine. Finally, calcium consumed together with iron-providing foodstuff inhibits iron absorption, whereas vitamins A and C improve it (Lynch, 1997). With respect to the role of infectious agents, it has been supported that iron-deficiency anemia results from an immune response that binds iron to prevent its use by infectious agents (Stuart-Macadam, 1992). However, although iron withholding may decrease the incidence and intensity of many infections, beyond a certain limit it actually increases host susceptibility to invading organisms (Weinberg, 1992; see also Hadley and DeCaro, 2015 for a lack of association between iron-deficiency anemia and low likelihood of infection). Regarding parasitic infections and their role in iron absorption, infection by whipworms and hookworms causes iron loss through intestinal bleeding, whereas parasites such as giardia and roundworm diminish the intestinal absorption of iron (Brooker et al., 2007; Stoltzfus et al., 1997). Finally, regarding the role of growth, infants require more iron than other age groups because of their high growth rate. As a result, maternal anemia during pregnancy increases the possibility of the offspring becoming anemic too (Allen, 1997).
|
|
|
Scooped by
Gilbert C FAURE
February 20, 2022 3:59 AM
|
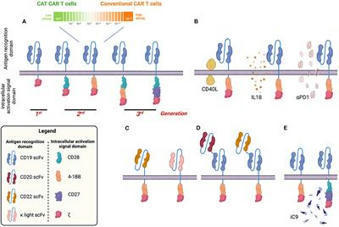
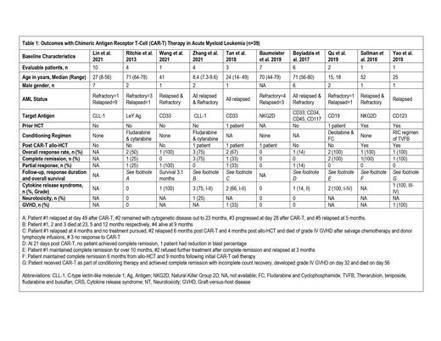
Chimeric antigen receptor T-cell therapy (CAR-T) targeting CD19 has been associated with remarkable responses in paediatric patients and adolescents and young adults (AYA) with relapsed/refractory (R/R) B-cell precursor acute lymphoblastic leukaemia (BCP-ALL).
|
|
Scooped by
Gilbert C FAURE
February 6, 2022 2:00 PM
|
Cure4Kids offers a variety of content, including disease- and treatment- specific seminars, written articles, and challenging image-based instruction. Both live and virtual instructor-led classes in multiple languages are offered to educate healthcare providers across the globe. Seminars can be searched by type of disease, treatment, or care provided. Some seminars are available for CME credit.
|
|
Scooped by
Gilbert C FAURE
February 6, 2022 12:07 PM
|
Minimal residual disease (MRD) has evolved as a sensitive and highly prognostic surrogate parameter of response to therapy in chronic lymphocytic leukemia (CLL). Multiple methods have been established to measure and quantify MRD during and after therapy.
|
|
Scooped by
Gilbert C FAURE
January 14, 2022 10:48 AM
|
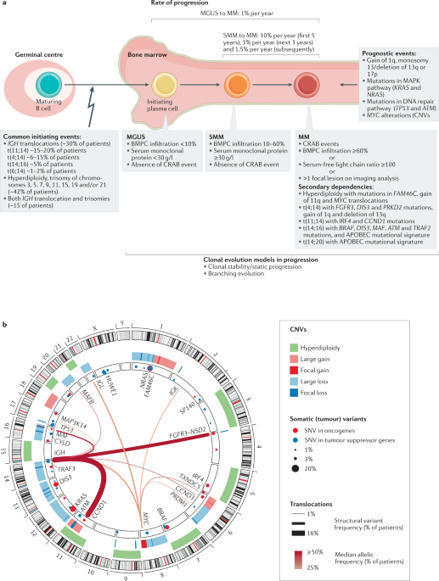
Multiple myeloma (MM) is a haematological malignancy of plasma cells characterized by substantial intraclonal genetic heterogeneity. Although therapeutic advances made in the past few years have led to improved outcomes and longer survival, MM remains largely incurable. Over the past decade, genomic analyses of patient samples have demonstrated that MM is not a single disease but rather a spectrum of haematological entities that all share similar clinical symptoms. Moreover, analyses of samples from monoclonal gammopathy of undetermined significance and smouldering MM have also shown the existence of genetic heterogeneity in precursor stages, in some cases remarkably similar to that of MM. This heterogeneity highlights the need for a greater dissection of underlying disease biology, especially the clonal diversity and molecular events underpinning MM at each stage to enable the stratification of individuals with a high risk of progression. Emerging single-cell sequencing technologies present a superlative solution to delineate the complexity of monoclonal gammopathy of undetermined significance, smouldering MM and MM. In this Review, we discuss how genomics has revealed novel insights into clonal evolution patterns of MM and provide examples from single-cell studies that are beginning to unravel the mutational and phenotypic characteristics of individual cells within the bone marrow tumour, immune microenvironment and peripheral blood. We also address future perspectives on clinical application, proposing that multi-omics single-cell profiling can guide early patient diagnosis, risk stratification and treatment strategies. Multiple myeloma and its precursor stages, monoclonal gammopathy of undetermined significance and smouldering multiple myeloma, have a considerable degree of genetic heterogeneity. The authors of this Review discuss how single-cell studies in these individuals are enabling the mutational and phenotypic characterization of cells within the bone marrow tumour, immune microenvironment and peripheral blood to eventually guide early diagnosis, risk stratification and treatment strategies.
|
|
Scooped by
Gilbert C FAURE
December 31, 2021 4:58 AM
|
emiaNet evaluated which aspects are crucial for accurate MFC-MRD measurement. Here, we report on the agreement, obtained via a combination of a cross-sectional questionnaire, live discussions, and a Delphi poll. The recommendations consist of several key issues from bone marrow sampling to final laboratory reporting to ensure quality and reproducibility of results. Furthermore, the experiences were tested by comparing two 8-color MRD panels in multiple laboratories. The results presented here underscore the feasibility and the utility of a harmonized theoretical and practical MFC-MRD assessment and are a next step toward furthe
|
|
Scooped by
Gilbert C FAURE
December 18, 2021 6:33 AM
|
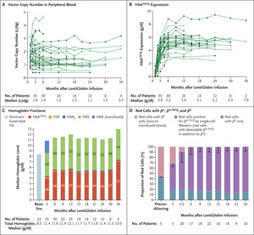
Original Article from The New England Journal of Medicine — Biologic and Clinical Efficacy of LentiGlobin for Sickle Cell Disease
|
|
Scooped by
Gilbert C FAURE
December 13, 2021 10:11 AM
|
The premier event in malignant and non-malignant hematology, the ASH annual meeting highlights the highest-caliber science and the most important areas of clinical progress in hematology.
|
|
Scooped by
Gilbert C FAURE
November 28, 2021 6:48 AM
|
Abstract. Background: Acute myeloid leukemia (AML) is a clonal hematologic malignancy that generally affects older adults.Despite achieving complete remission...
|
|
Scooped by
Gilbert C FAURE
November 28, 2021 5:24 AM
|
An abstract is unavailable.
|
|
Scooped by
Gilbert C FAURE
October 23, 2021 2:41 PM
|
Abstract Finally,after decades of stagnation, the therapeutic landscape for sickle cell disease (SCD) is changing with an increasing number of novel therapeutics. Hydroxyurea remains the primary di...
|
|
Scooped by
Gilbert C FAURE
October 9, 2021 10:51 AM
|
Kumar SK, et al. Multiple myeloma. Nat Rev Dis Primers. 2017;3:17046. View this article via: PubMed Google Scholar Cowan AJ, et al. Global burden of multiple myeloma: a systematic analysis for the Global Burden of Disease Study 2016. JAMA Oncol. 2018;4(9):1221–1227.View this article via: PubMed CrossRef Google Scholar Landgren O, et al. Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: a prospective study. Blood. 2009;113(22):5412–5417.View this article via: PubMed CrossRef Google Scholar Kyle RA, et al. Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med. 2006;354(13):1362–1369.View this article via: PubMed CrossRef Google Scholar Kyle RA, et al. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med. 2007;356(25):2582–2590.View this article via: PubMed CrossRef Google Scholar Manier S, Salem KZ, Park J, Landau DA, Getz G, Ghobrial IM. Genomic complexity of multiple myeloma and its clinical implications. Nat Rev Clin Oncol. 2017;14(2):100–113.View this article via: PubMed CrossRef Google Scholar Kuehl WM, Bergsagel PL. Molecular pathogenesis of multiple myeloma and its premalignant precursor. J Clin Invest. 2012;122(10):3456–3463.View this article via: JCI PubMed CrossRef Google Scholar Suen H, et al. Multiple myeloma causes clonal T-cell immunosenescence: identification of potential novel targets for promoting tumour immunity and implications for checkpoint blockade. Leukemia. 2016;30(8):1716–1724.View this article via: PubMed CrossRef Google Scholar Guillerey C, et al. TIGIT immune checkpoint blockade restores CD8+ T-cell immunity against multiple myeloma. Blood. 2018;132(16):1689–1694.View this article via: PubMed CrossRef Google Scholar Chung DJ, et al. T-cell exhaustion in multiple myeloma relapse after autotransplant: optimal timing of immunotherapy. Cancer Immunol Res. 2016;4(1):61–71.View this article via: PubMed CrossRef Google Scholar Zelle-Rieser C, et al. T cells in multiple myeloma display features of exhaustion and senescence at the tumor site. J Hematol Oncol. 2016;9(1):116. View this article via: PubMed CrossRef Google Scholar Yadav M, et al. Tigit, CD226 and PD-L1/PD-1 are highly expressed by marrow-infiltrating T cells in patients with multiple myeloma. Blood. 2016;128(22):2102. View this article via: CrossRef Google Scholar Dhodapkar MV, et al. A reversible defect in natural killer T cell function characterizes the progression of premalignant to malignant multiple myeloma. J Exp Med. 2003;197(12):1667–1676.View this article via: PubMed CrossRef Google Scholar Minnie SA, et al. Myeloma escape after stem cell transplantation is a consequence of T-cell exhaustion and is prevented by TIGIT blockade. Blood. 2018;132(16):1675–1688.View this article via: PubMed CrossRef Google Scholar Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331(6024):1565–1570.View this article via: PubMed CrossRef Google Scholar Walker BA, et al. Intraclonal heterogeneity is a critical early event in the development of myeloma and precedes the development of clinical symptoms. Leukemia. 2014;28(2):384–390.View this article via: PubMed CrossRef Google Scholar Dutta AK, et al. Subclonal evolution in disease progression from MGUS/SMM to multiple myeloma is characterised by clonal stability. Leukemia. 2019;33(2):457–468.View this article via: PubMed CrossRef Google Scholar Zhao S, et al. Serial exome analysis of disease progression in premalignant gammopathies. Leukemia. 2014;28(7):1548–1552.View this article via: PubMed CrossRef Google Scholar Mateos MV, et al. Lenalidomide plus dexamethasone for high-risk smoldering multiple myeloma. N Engl J Med. 2013;369(5):438–447.View this article via: PubMed CrossRef Google Scholar Lonial S, et al. Randomized trial of lenalidomide versus observation in smoldering multiple myeloma [published online October 25, 2019]. J Clin Oncol. https://doi.org/10.1200/JCO.19.01740. Dhodapkar MV, Krasovsky J, Osman K, Geller MD. Vigorous premalignancy-specific effector T cell response in the bone marrow of patients with monoclonal gammopathy. J Exp Med. 2003;198(11):1753–1757.View this article via: PubMed CrossRef Google Scholar Dhodapkar MV, Krasovsky J, Olson K. T cells from the tumor microenvironment of patients with progressive myeloma can generate strong, tumor-specific cytolytic responses to autologous, tumor-loaded dendritic cells. Proc Natl Acad Sci U S A. 2002;99(20):13009–13013.View this article via: PubMed CrossRef Google Scholar Hayashi T, et al. Ex vivo induction of multiple myeloma-specific cytotoxic T lymphocytes. Blood. 2003;102(4):1435–1442.View this article via: PubMed CrossRef Google Scholar Wen YJ, Min R, Tricot G, Barlogie B, Yi Q. Tumor lysate-specific cytotoxic T lymphocytes in multiple myeloma: promising effector cells for immunotherapy. Blood. 2002;99(9):3280–3285.View this article via: PubMed CrossRef Google Scholar Alexandrov LB, et al. Signatures of mutational processes in human cancer. Nature. 2013;500(7463):415–421.View this article via: PubMed CrossRef Google Scholar Vuckovic S, et al. Bone marrow transplantation generates T cell-dependent control of myeloma in mice. J Clin Invest. 2019;129(1):106–121.View this article via: JCI PubMed CrossRef Google Scholar Chesi M, et al. AID-dependent activation of a MYC transgene induces multiple myeloma in a conditional mouse model of post-germinal center malignancies. Cancer Cell. 2008;13(2):167–180.View this article via: PubMed CrossRef Google Scholar Gatza E, et al. Etanercept plus topical corticosteroids as initial therapy for grade one acute graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2014;20(9):1426–1434.View this article via: PubMed CrossRef Google Scholar Miller A, et al. High somatic mutation and neoantigen burden are correlated with decreased progression-free survival in multiple myeloma. Blood Cancer J. 2017;7(9):e612. View this article via: PubMed CrossRef Google Scholar Lohr JG, et al. Widespread genetic heterogeneity in multiple myeloma: implications for targeted therapy. Cancer Cell. 2014;25(1):91–101.View this article via: PubMed CrossRef Google Scholar Bailur JK, et al. Early alterations in stem-like/resident T cells, innate and myeloid cells in the bone marrow in preneoplastic gammopathy. JCI Insight. 2019;5:127807. View this article via: JCI Insight PubMed Google Scholar Carnaud C, et al. Cutting edge: Cross-talk between cells of the innate immune system: NKT cells rapidly activate NK cells. J Immunol. 1999;163(9):4647–4650.View this article via: PubMed Google Scholar Eberl G, MacDonald HR. Selective induction of NK cell proliferation and cytotoxicity by activated NKT cells. Eur J Immunol. 2000;30(4):985–992.View this article via: PubMed CrossRef Google Scholar Silk JD, et al. Utilizing the adjuvant properties of CD1d-dependent NK T cells in T cell-mediated immunotherapy. J Clin Invest. 2004;114(12):1800–1811.View this article via: JCI PubMed CrossRef Google Scholar Viey E, Laplace C, Escudier B. Peripheral γδ T-lymphocytes as an innovative tool in immunotherapy for metastatic renal cell carcinoma. Expert Rev Anticancer Ther. 2005;5(6):973–986.View this article via: PubMed CrossRef Google Scholar Corvaisier M, et al. Vγ9Vδ2 T cell response to colon carcinoma cells. J Immunol. 2005;175(8):5481–5488.View this article via: PubMed CrossRef Google Scholar Groh V, Rhinehart R, Secrist H, Bauer S, Grabstein KH, Spies T. Broad tumor-associated expression and recognition by tumor-derived γδ T cells of MICA and MICB. Proc Natl Acad Sci U S A. 1999;96(12):6879–6884.View this article via: PubMed CrossRef Google Scholar Fournié JJ, et al. What lessons can be learned from γδ T cell-based cancer immunotherapy trials? Cell Mol Immunol. 2013;10(1):35–41.View this article via: PubMed CrossRef Google Scholar Zocchi MR, Poggi A. Role of γδ T lymphocytes in tumor defense. Front Biosci. 2004;9:2588–2604.View this article via: PubMed CrossRef Google Scholar Carbone E, et al. HLA class I, NKG2D, and natural cytotoxicity receptors regulate multiple myeloma cell recognition by natural killer cells. Blood. 2005;105(1):251–258.View this article via: PubMed CrossRef Google Scholar Dhodapkar MV, Richter J. Harnessing natural killer T (NKT) cells in human myeloma: progress and challenges. Clin Immunol. 2011;140(2):160–166.View this article via: PubMed CrossRef Google Scholar Guillerey C, et al. Immunosurveillance and therapy of multiple myeloma are CD226 dependent. J Clin Invest. 2015;125(5):2077–2089.View this article via: JCI PubMed CrossRef Google Scholar Osterborg A, Nilsson B, Björkholm M, Holm G, Mellstedt H. Natural killer cell activity in monoclonal gammopathies: relation to disease activity. Eur J Haematol. 1990;45(3):153–157.View this article via: PubMed Google Scholar Paiva B, et al. Immune status of high-risk smoldering multiple myeloma patients and its therapeutic modulation under LenDex: a longitudinal analysis. Blood. 2016;127(9):1151–1162.View this article via: PubMed CrossRef Google Scholar Davies FE, et al. Thalidomide and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple myeloma. Blood. 2001;98(1):210–216.View this article via: PubMed CrossRef Google Scholar Hayashi T, et al. Molecular mechanisms whereby immunomodulatory drugs activate natural killer cells: clinical application. Br J Haematol. 2005;128(2):192–203.View this article via: PubMed CrossRef Google Scholar Fedele PL, et al. IMiDs prime myeloma cells for daratumumab-mediated cytotoxicity through loss of Ikaros and Aiolos. Blood. 2018;132(20):2166–2178.View this article via: PubMed CrossRef Google Scholar Campbell KS, Cohen AD, Pazina T. Mechanisms of NK cell activation and clinical activity of the therapeutic SLAMF7 antibody, elotuzumab in multiple myeloma. Front Immunol. 2018;9:2551. View this article via: PubMed Google Scholar Mittal D, Gubin MM, Schreiber RD, Smyth MJ. New insights into cancer immunoediting and its three component phases — elimination, equilibrium and escape. Curr Opin Immunol. 2014;27:16–25.View this article via: PubMed CrossRef Google Scholar Guillerey C, Nakamura K, Vuckovic S, Hill GR, Smyth MJ. Immune responses in multiple myeloma: role of the natural immune surveillance and potential of immunotherapies. Cell Mol Life Sci. 2016;73(8):1569–1589.View this article via: PubMed CrossRef Google Scholar Crespo J, Sun H, Welling TH, Tian Z, Zou W. T cell anergy, exhaustion, senescence, and stemness in the tumor microenvironment. Curr Opin Immunol. 2013;25(2):214–221.View this article via: PubMed CrossRef Google Scholar Blank CU, et al. Defining ‘T cell exhaustion’. Nat Rev Immunol. 2019;19(11):665–674.View this article via: PubMed CrossRef Google Scholar Wherry EJ, Kurachi M. Molecular and cellular insights into T cell exhaustion. Nat Rev Immunol. 2015;15(8):486–499.View this article via: PubMed CrossRef Google Scholar Rosenblatt J, et al. PD-1 blockade by CT-011, anti-PD-1 antibody, enhances ex vivo T-cell responses to autologous dendritic cell/myeloma fusion vaccine. J Immunother. 2011;34(5):409–418.View this article via: PubMed CrossRef Google Scholar Palumbo A, Bruno B, Boccadoro M, Pileri A. Interferon-gamma in multiple myeloma. Leuk Lymphoma. 1995;18(3–4):215–219.View this article via: PubMed Google Scholar Yousef S, et al. Immunomodulatory molecule PD-L1 is expressed on malignant plasma cells and myeloma-propagating pre-plasma cells in the bone marrow of multiple myeloma patients. Blood Cancer J. 2015;5:e285. View this article via: PubMed Google Scholar El-Sherbiny YM, et al. The requirement for DNAM-1, NKG2D, and NKp46 in the natural killer cell-mediated killing of myeloma cells. Cancer Res. 2007;67(18):8444–8449.View this article via: PubMed CrossRef Google Scholar Bahlis NJ, et al. CD28-mediated regulation of multiple myeloma cell proliferation and survival. Blood. 2007;109(11):5002–5010.View this article via: PubMed CrossRef Google Scholar Ishibashi M, et al. Myeloma drug resistance induced by binding of myeloma B7-H1 (PD-L1) to PD-1. Cancer Immunol Res. 2016;4(9):779–788.View this article via: PubMed CrossRef Google Scholar Wang L, et al. Serum levels of soluble programmed death ligand 1 predict treatment response and progression free survival in multiple myeloma. Oncotarget. 2015;6(38):41228–41236.View this article via: PubMed Google Scholar Fauriat C, Mallet F, Olive D, Costello RT. Impaired activating receptor expression pattern in natural killer cells from patients with multiple myeloma. Leukemia. 2006;20(4):732–733.View this article via: PubMed CrossRef Google Scholar Benson DM, et al. The PD-1/PD-L1 axis modulates the natural killer cell versus multiple myeloma effect: a therapeutic target for CT-011, a novel monoclonal anti-PD-1 antibody. Blood. 2010;116(13):2286–2294.View this article via: PubMed CrossRef Google Scholar Ratta M, et al. Dendritic cells are functionally defective in multiple myeloma: the role of interleukin-6. Blood. 2002;100(1):230–237.View this article via: PubMed CrossRef Google Scholar Bahlis NJ, et al. CD28-mediated regulation of multiple myeloma cell proliferation and survival. Blood. 2007;109(11):5002–5010.View this article via: PubMed CrossRef Google Scholar Murray ME, et al. CD28-mediated pro-survival signaling induces chemotherapeutic resistance in multiple myeloma. Blood. 2014;123(24):3770–3779.View this article via: PubMed CrossRef Google Scholar Kukreja A, et al. Enhancement of clonogenicity of human multiple myeloma by dendritic cells. J Exp Med. 2006;203(8):1859–1865.View this article via: PubMed CrossRef Google Scholar Leone P, et al. Dendritic cells accumulate in the bone marrow of myeloma patients where they protect tumor plasma cells from CD8+ T-cell killing. Blood. 2015;126(12):1443–1451.View this article via: PubMed CrossRef Google Scholar Racanelli V, et al. Alterations in the antigen processing-presenting machinery of transformed plasma cells are associated with reduced recognition by CD8+ T cells and characterize the progression of MGUS to multiple myeloma. Blood. 2010;115(6):1185–1193.View this article via: PubMed CrossRef Google Scholar Chomarat P, Banchereau J, Davoust J, Palucka AK. IL-6 switches the differentiation of monocytes from dendritic cells to macrophages. Nat Immunol. 2000;1(6):510–514.View this article via: PubMed CrossRef Google Scholar van Zaanen HC, et al. Endogenous interleukin 6 production in multiple myeloma patients treated with chimeric monoclonal anti-IL6 antibodies indicates the existence of a positive feed-back loop. J Clin Invest. 1996;98(6):1441–1448.View this article via: JCI PubMed CrossRef Google Scholar Hilbert DM, Kopf M, Mock BA, Köhler G, Rudikoff S. Interleukin 6 is essential for in vivo development of B lineage neoplasms. J Exp Med. 1995;182(1):243–248.View this article via: PubMed CrossRef Google Scholar Serody JS, Hill GR. The IL-17 differentiation pathway and its role in transplant outcome. Biol Blood Marrow Transplant. 2012;18(1 suppl):S56–S61.View this article via: PubMed Google Scholar Bettelli E, et al. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature. 2006;441(7090):235–238.View this article via: PubMed CrossRef Google Scholar Veldhoen M, Hocking RJ, Atkins CJ, Locksley RM, Stockinger B. TGF-β in the context of an inflammatory cytokine milieu supports de novo differentiation of IL-17-producing T cells. Immunity. 2006;24(2):179–189.View this article via: PubMed CrossRef Google Scholar Prabhala RH, et al. Elevated IL-17 produced by TH17 cells promotes myeloma cell growth and inhibits immune function in multiple myeloma. Blood. 2010;115(26):5385–5392.View this article via: PubMed CrossRef Google Scholar Prabhala RH, et al. Targeting IL-17A in multiple myeloma: a potential novel therapeutic approach in myeloma. Leukemia. 2016;30(2):379–389.View this article via: PubMed CrossRef Google Scholar Li Y, et al. Potential relationship and clinical significance of miRNAs and Th17 cytokines in patients with multiple myeloma. Leuk Res. 2014;38(9):1130–1135.View this article via: PubMed CrossRef Google Scholar Alexandrakis MG, et al. Serum interleukin-17 and its relationship to angiogenic factors in multiple myeloma. Eur J Intern Med. 2006;17(6):412–416.View this article via: PubMed CrossRef Google Scholar Calcinotto A, et al. Microbiota-driven interleukin-17-producing cells and eosinophils synergize to accelerate multiple myeloma progression. Nat Commun. 2018;9(1):4832. View this article via: PubMed CrossRef Google Scholar Aras S, Zaidi MR. TAMeless traitors: macrophages in cancer progression and metastasis. Br J Cancer. 2017;117(11):1583–1591.View this article via: PubMed CrossRef Google Scholar Lin EY, Nguyen AV, Russell RG, Pollard JW. Colony-stimulating factor 1 promotes progression of mammary tumors to malignancy. J Exp Med. 2001;193(6):727–740.View this article via: PubMed CrossRef Google Scholar Ries CH, et al. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014;25(6):846–859.View this article via: PubMed CrossRef Google Scholar Ao JY, et al. Colony-stimulating factor 1 receptor blockade inhibits tumor growth by altering the polarization of tumor-associated macrophages in hepatocellular carcinoma. Mol Cancer Ther. 2017;16(8):1544–1554.View this article via: PubMed CrossRef Google Scholar Wang Q, et al. Therapeutic effects of CSF1R-blocking antibodies in multiple myeloma. Leukemia. 2018;32(1):176–183.View this article via: PubMed CrossRef Google Scholar Zheng Y, et al. Macrophages are an abundant component of myeloma microenvironment and protect myeloma cells from chemotherapy drug-induced apoptosis. Blood. 2009;114(17):3625–3628.View this article via: PubMed CrossRef Google Scholar Nakamura K, et al. Dysregulated IL-18 is a key driver of immunosuppression and a possible therapeutic target in the multiple myeloma microenvironment. Cancer Cell. 2018;33(4):634–648.e5.View this article via: PubMed CrossRef Google Scholar Lesokhin AM, et al. Nivolumab in patients with relapsed or refractory hematologic malignancy: preliminary results of a phase Ib study. J Clin Oncol. 2016;34(23):2698–2704.View this article via: PubMed CrossRef Google Scholar Jing W, et al. Combined immune checkpoint protein blockade and low dose whole body irradiation as immunotherapy for myeloma. J Immunother Cancer. 2015;3(1):2. View this article via: PubMed CrossRef Google Scholar Hallett WH, Jing W, Drobyski WR, Johnson BD. Immunosuppressive effects of multiple myeloma are overcome by PD-L1 blockade. Biol Blood Marrow Transplant. 2011;17(8):1133–1145.View this article via: PubMed CrossRef Google Scholar Kearl TJ, Jing W, Gershan JA, Johnson BD. Programmed death receptor-1/programmed death receptor ligand-1 blockade after transient lymphodepletion to treat myeloma. J Immunol. 2013;190(11):5620–5628.View this article via: PubMed CrossRef Google Scholar D’Souza A, et al. A phase 2 study of pembrolizumab during lymphodepletion after autologous hematopoietic cell transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2019;25(8):1492–1497.View this article via: PubMed CrossRef Google Scholar Du X, et al. A reappraisal of CTLA-4 checkpoint blockade in cancer immunotherapy. Cell Res. 2018;28(4):416–432.View this article via: PubMed CrossRef Google Scholar Arce Vargas F, et al. Fc Effector function contributes to the activity of human anti-CTLA-4 antibodies. Cancer Cell. 2018;33(4):649–663.e4.View this article via: PubMed CrossRef Google Scholar Yonezawa A, Dutt S, Chester C, Kim J, Kohrt HE. Boosting cancer immunotherapy with anti-CD137 antibody therapy. Clin Cancer Res. 2015;21(14):3113–3120.View this article via: PubMed CrossRef Google Scholar Murillo O, et al. Therapeutic antitumor efficacy of anti-CD137 agonistic monoclonal antibody in mouse models of myeloma. Clin Cancer Res. 2008;14(21):6895–6906.View this article via: PubMed CrossRef Google Scholar McKee SJ, Doff BL, Soon MS, Mattarollo SR. Therapeutic efficacy of 4-1BB costimulation is abrogated by PD-1 blockade in a model of spontaneous B-cell lymphoma. Cancer Immunol Res. 2017;5(3):191–197.View this article via: PubMed CrossRef Google Scholar Krönke J, et al. Lenalidomide causes selective degradation of IKZF1 and IKZF3 in multiple myeloma cells. Science. 2014;343(6168):301–305.View this article via: PubMed CrossRef Google Scholar Lu G, et al. The myeloma drug lenalidomide promotes the cereblon-dependent destruction of Ikaros proteins. Science. 2014;343(6168):305–309.View this article via: PubMed CrossRef Google Scholar Fink EC, et al. CrbnI391V is sufficient to confer in vivo sensitivity to thalidomide and its derivatives in mice. Blood. 2018;132(14):1535–1544.View this article via: PubMed CrossRef Google Scholar Quach H, et al. Mechanism of action of immunomodulatory drugs (IMiDS) in multiple myeloma. Leukemia. 2010;24(1):22–32.View this article via: PubMed CrossRef Google Scholar Luptakova K, et al. Lenalidomide enhances anti-myeloma cellular immunity. Cancer Immunol Immunother. 2013;62(1):39–49.View this article via: PubMed CrossRef Google Scholar Galustian C, et al. The anti-cancer agents lenalidomide and pomalidomide inhibit the proliferation and function of T regulatory cells. Cancer Immunol Immunother. 2009;58(7):1033–1045.View this article via: PubMed CrossRef Google Scholar Dimopoulos MA, et al. Elotuzumab plus pomalidomide and dexamethasone for multiple myeloma. N Engl J Med. 2018;379(19):1811–1822.View this article via: PubMed CrossRef Google Scholar Görgün G, et al. Lenalidomide enhances immune checkpoint blockade-induced immune response in multiple myeloma. Clin Cancer Res. 2015;21(20):4607–4618.View this article via: PubMed CrossRef Google Scholar Badros A, et al. Pembrolizumab, pomalidomide, and low-dose dexamethasone for relapsed/refractory multiple myeloma. Blood. 2017;130(10):1189–1197.View this article via: PubMed CrossRef Google Scholar Ocio EM, et al. Pembrolizumab (Pembro) plus lenalidomide (Len) and low-dose dexamethasone (Dex) for relapsed/refractory multiple myeloma (RRMM) efficacy and biomarker analyses. J Clin Oncol. 2017;35(15 suppl):8015. View this article via: CrossRef Google Scholar Gormley NJ, Pazdur R. Immunotherapy combinations in multiple myeloma — known unknowns. N Engl J Med. 2018;379(19):1791–1795.View this article via: PubMed CrossRef Google Scholar Bezman NA, et al. PD-1 blockade enhances elotuzumab efficacy in mouse tumor models. Blood Adv. 2017;1(12):753–765.View this article via: PubMed CrossRef Google Scholar Dimopoulos MA, et al. Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(14):1319–1331.View this article via: PubMed CrossRef Google Scholar Palumbo A, et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(8):754–766.View this article via: PubMed CrossRef Google Scholar Krejcik J, et al. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood. 2016;128(3):384–394.View this article via: PubMed CrossRef Google Scholar Bezman NA, et al. Abstract 1727: Antitumor activity associated with dual targeting of CD38 and programmed death-1 (PD-1) pathways in preclinical models. Cancer Res. 2018;78(suppl 13):1727. View this article via: CrossRef Google Scholar Thirukkumaran CM, et al. Oncolytic immunotherapy and bortezomib synergy improves survival of refractory multiple myeloma in a preclinical model. Blood Adv. 2019;3(5):797–812.View this article via: PubMed CrossRef Google Scholar Müller LME, et al. Abstract 18: Evaluating the contribution of anti-myeloma immunity for the efficacy of oncolytic reovirus therapy. Clin Cancer Res. 2017;23(suppl 24):18. View this article via: CrossRef Google Scholar Parrish C, Scott GB, Coffey M, Melcher A, Errington-Mais F, Cook G. Combination therapy with reovirus and immunomodulatory drugs induces direct oncolytic and immune-mediated killing of multiple myeloma cells and overcomes stromal-mediated microenvironmental protection. Blood. 2014;124(21):4778. View this article via: CrossRef Google Scholar Attal M, et al. Autologous transplantation for multiple myeloma in the era of new drugs: a phase III study of the Intergroupe Francophone Du Myelome (IFM/DFCI 2009 Trial). Blood. 2015;126(23):391. View this article via: CrossRef Google Scholar Cavo M, et al. Bortezomib with thalidomide plus dexamethasone compared with thalidomide plus dexamethasone as induction therapy before, and consolidation therapy after, double autologous stem-cell transplantation in newly diagnosed multiple myeloma: a randomised phase 3 study. Lancet. 2010;376(9758):2075–2085.View this article via: PubMed CrossRef Google Scholar Attal M, et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Français du Myélome. N Engl J Med. 1996;335(2):91–97.View this article via: PubMed CrossRef Google Scholar Child JA, et al. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348(19):1875–1883.View this article via: PubMed CrossRef Google Scholar Bensinger WI. Role of autologous and allogeneic stem cell transplantation in myeloma. Leukemia. 2009;23(3):442–448.View this article via: PubMed CrossRef Google Scholar Martinez-Lopez J, et al. Long-term prognostic significance of response in multiple myeloma after stem cell transplantation. Blood. 2011;118(3):529–534.View this article via: PubMed CrossRef Google Scholar Lu X, et al. Alkylating agent melphalan augments the efficacy of adoptive immunotherapy using tumor-specific CD4+ T cells. J Immunol. 2015;194(4):2011–2021.View this article via: PubMed CrossRef Google Scholar Olsen GA, Gockerman JP, Bast RC, Borowitz M, Peters WP. Altered immunologic reconstitution after standard-dose chemotherapy or high-dose chemotherapy with autologous bone marrow support. Transplantation. 1988;46(1):57–60.View this article via: PubMed CrossRef Google Scholar Aschan J, Lönnqvist B, Ringdén O, Kumlien G, Gahrton G. Graft-versus-myeloma effect. Lancet. 1996;348(9023):346. View this article via: PubMed Google Scholar Tricot G, Vesole DH, Jagannath S, Hilton J, Munshi N, Barlogie B. Graft-versus-myeloma effect: proof of principle. Blood. 1996;87(3):1196–1198.View this article via: PubMed CrossRef Google Scholar Halapi E, et al. T cell repertoire in patients with multiple myeloma and monoclonal gammopathy of undetermined significance: clonal CD8+ T cell expansions are found preferentially in patients with a low tumor burden. Eur J Immunol. 1997;27(9):2245–2252.View this article via: PubMed CrossRef Google Scholar Helg C, Starobinski M, Jeannet M, Chapuis B. Donor lymphocyte infusion for the treatment of relapse after allogeneic hematopoietic stem cell transplantation. Leuk Lymphoma. 1998;29(3–4):301–313.View this article via: PubMed Google Scholar Yin X, Tang L, Fan F, Jiang Q, Sun C, Hu Y. Allogeneic stem-cell transplantation for multiple myeloma: a systematic review and meta-analysis from 2007 to 2017. Cancer Cell Int. 2018;18:62. View this article via: PubMed Google Scholar Noonan KA, Borrello IM. Marrow infiltrating lymphocytes: their role in adoptive immunotherapy. Cancer J. 2015;21(6):501–505.View this article via: PubMed CrossRef Google Scholar Noonan KA, et al. Adoptive transfer of activated marrow-infiltrating lymphocytes induces measurable antitumor immunity in the bone marrow in multiple myeloma. Sci Transl Med. 2015;7(288):288ra78. View this article via: PubMed CrossRef Google Scholar Yu X, et al. The surface protein TIGIT suppresses T cell activation by promoting the generation of mature immunoregulatory dendritic cells. Nat Immunol. 2009;10(1):48–57.View this article via: PubMed CrossRef Google Scholar Leroy X, et al. Abstract LB-114: a-TIGIT antagonist antibody EOS884448 shows dual mechanism of action by restoration of T cell effector functions and preferential depletion of Treg. Cancer Res. 2018;78(suppl 13):LB-114-LB-114. View this article via: CrossRef Google Scholar Hoyos V, Borrello I. The immunotherapy era of myeloma: monoclonal antibodies, vaccines, and adoptive T-cell therapies. Blood. 2016;128(13):1679–1687.View this article via: PubMed CrossRef Google Scholar Yi Q, Desikan R, Barlogie B, Munshi N. Optimizing dendritic cell-based immunotherapy in multiple myeloma. Br J Haematol. 2002;117(2):297–305.View this article via: PubMed CrossRef Google Scholar Curti A, et al. Phase I/II clinical trial of sequential subcutaneous and intravenous delivery of dendritic cell vaccination for refractory multiple myeloma using patient-specific tumour idiotype protein or idiotype (VDJ)-derived class I-restricted peptides. Br J Haematol. 2007;139(3):415–424.View this article via: PubMed CrossRef Google Scholar Reichardt VL, et al. Idiotype vaccination using dendritic cells after autologous peripheral blood stem cell transplantation for multiple myeloma — a feasibility study. Blood. 1999;93(7):2411–2419.View this article via: PubMed Google Scholar Rapoport AP, et al. Combination immunotherapy after ASCT for multiple myeloma using MAGE-A3/Poly-ICLC immunizations followed by adoptive transfer of vaccine-primed and costimulated autologous T cells. Clin Cancer Res. 2014;20(5):1355–1365.View this article via: PubMed CrossRef Google Scholar Nahas MR, Rosenblatt J, Lazarus HM, Avigan D. Anti-cancer vaccine therapy for hematologic malignancies: an evolving era. Blood Rev. 2018;32(4):312–325.View this article via: PubMed CrossRef Google Scholar Brimnes MK, et al. Increased level of both CD4+FOXP3+ regulatory T cells and CD14+HLA-DR–/low myeloid-derived suppressor cells and decreased level of dendritic cells in patients with multiple myeloma. Scand J Immunol. 2010;72(6):540–547.View this article via: PubMed CrossRef Google Scholar Rosenblatt J, et al. Vaccination with dendritic cell/tumor fusions following autologous stem cell transplant induces immunologic and clinical responses in multiple myeloma patients. Clin Cancer Res. 2013;19(13):3640–3648.View this article via: PubMed CrossRef Google Scholar Rosenblatt J, et al. Vaccination with dendritic cell/tumor fusion cells results in cellular and humoral antitumor immune responses in patients with multiple myeloma. Blood. 2011;117(2):393–402.View this article via: PubMed CrossRef Google Scholar Avigan D, Rosenblatt J. Vaccine therapy in hematologic malignancies. Blood. 2018;131(24):2640–2650.View this article via: PubMed CrossRef Google Scholar Reichardt VL, Milazzo C, Brugger W, Einsele H, Kanz L, Brossart P. Idiotype vaccination of multiple myeloma patients using monocyte-derived dendritic cells. Haematologica. 2003;88(10):1139–1149.View this article via: PubMed Google Scholar Rhee Fv . Idiotype vaccination strategies in myeloma: how to overcome a dysfunctional immune system. Clin Cancer Res. 2007;13(5):1353–1355.View this article via: PubMed CrossRef Google Scholar Lacy MQ, et al. Idiotype-pulsed antigen-presenting cells following autologous transplantation for multiple myeloma may be associated with prolonged survival. Am J Hematol. 2009;84(12):799–802.View this article via: PubMed CrossRef Google Scholar Zuch de Zafra CL, et al. Targeting multiple myeloma with AMG 424, a novel anti-CD38/CD3 bispecific T-cell-recruiting antibody optimized for cytotoxicity and cytokine release. Clin Cancer Res. 2019;25(13):3921–3933.View this article via: PubMed CrossRef Google Scholar Demichelis-Gómez R, Pérez-Sámano D, Bourlon C. Bispecific antibodies in hematologic malignancies: when, to whom, and how should be best used? Curr Oncol Rep. 2019;21(2):17. View this article via: PubMed CrossRef Google Scholar Topp MS, et al. Evaluation of AMG 420, an anti-BCMA bispecific T-cell engager (BiTE) immunotherapy, in R/R multiple myeloma (MM) patients: updated results of a first-in-human (FIH) phase I dose escalation study. J Clin Oncol. 2019;37(suppl 15):8007. View this article via: CrossRef Google Scholar Cho S-F, et al. Anti-BCMA BiTE AMG 701 potently induces specific T cell lysis of human multiple myeloma (MM) cells and immunomodulation in the bone marrow microenvironment. Blood. 2018;132(suppl 1):592. View this article via: CrossRef Google Scholar Cho SF, et al. AMG 701 potently induces anti-multiple myeloma (MM) functions of T cells and IMiDs further enhance its efficacy to prevent MM relapse in vivo. Blood. 2019;134(suppl 1):135. View this article via: CrossRef Google Scholar Costa LJ, et al. First clinical study of the B-cell maturation antigen (BCMA) 2+1 T cell engager (TCE) CC-93269 in patients (Pts) with relapsed/refractory multiple myeloma (RRMM): interim results of a phase 1 multicenter trial. Blood. 2019;134(suppl 1):143. View this article via: CrossRef Google Scholar Frigault MJ, Maus MV. State of the art in CAR T cell therapy for CD19+ B cell malignancies. J Clin Invest. 2020;130(4):1586–1594. Sidana S, Shah N. CAR T-cell therapy: is it prime time in myeloma? Blood Adv. 2019;3(21):3473–3480.View this article via: PubMed Google Scholar O’Connor BP, et al. BCMA is essential for the survival of long-lived bone marrow plasma cells. J Exp Med. 2004;199(1):91–98.View this article via: PubMed CrossRef Google Scholar Friedman KM, et al. Effective targeting of multiple B-cell maturation antigen-expressing hematological malignances by anti-B-cell maturation antigen chimeric antigen receptor T cells. Hum Gene Ther. 2018;29(5):585–601.View this article via: PubMed CrossRef Google Scholar Brudno JN, et al. T cells genetically modified to express an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of poor-prognosis relapsed multiple myeloma. J Clin Oncol. 2018;36(22):2267–2280.View this article via: PubMed CrossRef Google Scholar Raje N, et al. Anti-BCMA CAR T-cell therapy bb2121 in relapsed or refractory multiple myeloma. N Engl J Med. 2019;380(18):1726–1737.View this article via: PubMed CrossRef Google Scholar Cohen AD, et al. B cell maturation antigen-specific CAR T cells are clinically active in multiple myeloma. J Clin Invest. 2019;129(6):2210–2221.View this article via: JCI PubMed CrossRef Google Scholar Sun C, et al. Safety and efficacy of targeting CD138 with a chimeric antigen receptor for the treatment of multiple myeloma. Oncotarget. 2019;10(24):2369–2383.View this article via: PubMed Google Scholar Gogishvili T, et al. SLAMF7-CAR T cells eliminate myeloma and confer selective fratricide of SLAMF7+ normal lymphocytes. Blood. 2017;130(26):2838–2847.View this article via: PubMed CrossRef Google Scholar Smith EL, et al. GPRC5D is a target for the immunotherapy of multiple myeloma with rationally designed CAR T cells. Sci Transl Med. 2019;11(485):eaau7746. View this article via: PubMed CrossRef Google Scholar McLellan AD, Ali Hosseini Rad SM. Chimeric antigen receptor T cell persistence and memory cell formation. Immunol Cell Biol. 2019;97(7):664–674.View this article via: PubMed CrossRef Google Scholar Fraietta JA, et al. Determinants of response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic lymphocytic leukemia. Nat Med. 2018;24(5):563–571.View this article via: PubMed CrossRef Google Scholar Green DJ, et al. Fully human Bcma targeted chimeric antigen receptor T cells administered in a defined composition demonstrate potency at low doses in advanced stage high risk multiple myeloma. Blood. 2018;132(suppl 1):1011. View this article via: CrossRef Google Scholar Cohen AD, Raje N, Fowler JA, Mezzi K, Scott EC, Dhodapkar MV. How to train your T cells: overcoming immune dysfunction in multiple myeloma. [published online ahead of print October 31, 2019]. Clin Cancer Res. https://doi.org/10.1158/1078-0432.CCR-19-2111. View this article via: PubMed CrossRef Google Scholar Garfall AL, et al. T-cell phenotypes associated with effective CAR T-cell therapy in postinduction vs relapsed multiple myeloma. Blood Adv. 2019;3(19):2812–2815.View this article via: PubMed CrossRef Google Scholar Shi X, et al. Tandom autologous transplantation and combined infusion of CD19 and Bcma-specific chimeric antigen receptor T cells for high risk MM: initial safety and efficacy report from a clinical pilot study. Blood. 2018;132(suppl 1):1009. View this article via: CrossRef Google Scholar Garfall AL, et al. Anti-CD19 CAR T cells with high-dose melphalan and autologous stem cell transplantation for refractory multiple myeloma. JCI Insight. 2018;3(8):120505. View this article via: JCI Insight PubMed Google Scholar Shah NN, Fry TJ. Mechanisms of resistance to CAR T cell therapy. Nat Rev Clin Oncol. 2019;16(6):372–385.View this article via: PubMed CrossRef Google Scholar Lynn RC, et al. c-Jun overexpression in CAR T cells induces exhaustion resistance. Nature. 2019;576(7786):293–300.View this article via: PubMed CrossRef Google Scholar van der Stegen SJ, Hamieh M, Sadelain M. The pharmacology of second-generation chimeric antigen receptors. Nat Rev Drug Discov. 2015;14(7):499–509.View this article via: PubMed CrossRef Google Scholar Kawalekar OU, et al. Distinct signaling of coreceptors regulates specific metabolism pathways and impacts memory development in CAR T cells. Immunity. 2016;44(2):380–390.View this article via: PubMed CrossRef Google Scholar Zhao Z, et al. Structural design of engineered costimulation determines tumor rejection kinetics and persistence of CAR T cells. Cancer Cell. 2015;28(4):415–428.View this article via: PubMed CrossRef Google Scholar Pont MJ, et al. γ-Secretase inhibition increases efficacy of BCMA-specific chimeric antigen receptor T cells in multiple myeloma. Blood. 2019;134(19):1585–1597.View this article via: PubMed CrossRef Google Scholar Jiao S, et al. Differences in tumor microenvironment dictate T helper lineage polarization and response to immune checkpoint therapy. Cell. 2019;179(5):1177–1190.e13.View this article via: PubMed CrossRef Google Scholar
|
|
Scooped by
Gilbert C FAURE
September 2, 2021 8:37 AM
|
Multidisciplinary Chronic Lymphocytic Leukemia Care Chronic lymphocytic leukemia (CLL) is a cancer of the B-lymphocytes that may be found in the bone marrow, blood, lymph nodes, spleen and sometimes other organs. CLL is the most common leukemia in adults and accounts for one quarter of new leukemia cases annually. The average age at diagnosis is 70, and CLL is rarely seen in those under the age of 40. CLL is considered a chronic disease because it can persist for a long time and often reoccurs over the lifetime of the patient. A less commonly seen cancer, CLL accounts for 1.2% of all cancers. For 2018, the American Cancer Society estimates that the U.S. will see about 20,940 new cases of chronic lymphocytic leukemia. CLL is often slow growing or indolent and symptomless, and is typically found accidentally during routine blood tests. Depending on many factors, many patients are put on a "watch and wait" treatment approach and are followed by their hematologist/oncologist and primary care provider until symptoms become significant and require treatment. Many clinical trials are exploring the efficacy of starting treatment before symptoms present. Explore practical resources to implement in your cancer program or practice today. If you are interested in learning more about this project, please contact Limaya Atembina, MSW, Program Manager, ACCC Provider Education.
|