 Your new post is loading...

|
Scooped by
rob halkes
March 5, 2014 8:54 AM
|
Background: Few studies have evaluated both the overall effect of ICU telemedicine programs and the effect of individual components of the intervention on clinical outcomes.
Methods: The effects of nonrandomized ICU telemedicine interventions on crude and adjusted mortality and length of stay (LOS) were measured. Additionally, individual intervention components related to process and setting of care were evaluated for their association with mortality and LOS.
Results: Overall, 118,990 adult patients (11,558 control subjects, 107,432 intervention group patients) from 56 ICUs in 32 hospitals from 19 US health-care systems were included. After statistical adjustment, hospital (hazard ratio [HR] = 0.84; 95% CI, 0.78-0.89; P < .001) and ICU (HR = 0.74; 95% CI, 0.68-0.79; P < .001) mortality in the ICU telemedicine intervention group was significantly better than that of control subjects. Moreover, adjusted hospital LOS was reduced, on average, by 0.5 (95% CI, 0.4-0.5), 1.0 (95% CI, 0.7-1.3), and 3.6 (95% CI, 2.3-4.8) days, and adjusted ICU LOS was reduced by 1.1 (95% CI, 0.8-1.4), 2.5 (95% CI, 1.6-3.4), and 4.5 (95% CI, 1.5-7.2) days among those who stayed in the ICU for ≥ 7, ≥ 14, and ≥ 30 days, respectively. Individual components of the interventions that were associated with lower mortality, reduced LOS, or both included (1) intensivist case review within 1 h of admission, (2) timely use of performance data, (3) adherence to ICU best practices, and (4) quicker alert response times.
Conclusions: ICU telemedicine interventions, specifically interventions that increase early intensivist case involvement, improve adherence to ICU best practices, reduce response times to alarms, and encourage the use of performance data, were associated with lower mortality and LOS.
|
|
Scooped by
rob halkes
February 21, 2014 10:51 AM
|
As England’s population both expands and ages, so the demands on primary care will grow. Within the current commissioning and funding system innovative models of primary care provision are already being used. This report describes examples of these through four case studies in different areas of England. It also highlights how the existing system is imperfectly understood, particularly regarding contracts. Building on ideas articulated in previous work, the report argues for a new approach that brings together funding for general practice with funding for many other services. It would entail new forms of commissioning, with GPs innovating in how care is delivered. Over time, the report foresees ‘family care networks’ emerging that provide forms of care well beyond what is currently available in general practices. Key findings - Demographic changes, increasing multi-morbidity, clusters of risk factors and the rising needs of frail older people are piling pressure on primary care.
- General practice is well placed to respond to these pressures, due to its registered list of patients. This permits practices both to tailor treatment and act preventively.
- When developing integrated community services, there must be engagement with social services to help people stay independent and out of hospital. Making high standard out-of-hospital services available 24/7 is essential to halting the rising use of hospitals.
- Currently practices cannot fully meet their ambitions to develop innovative care due to challenges posed by structural instability, shifting accountabilities, provider engagement and payment models.
- The case studies demonstrate considerable innovation within the current system, but also great complexity and instability. Organisational change and loss of organisational memory compound this. Technicalities of contracting are imperfectly understood, inhibiting the flexibility that already exists.
Policy implications - A rapid, radical shift is needed from the current model of general practice to the use of federations and networks of practices able to work on the scale required for effective integration of services.
- Without changes to commissioning and funding arrangements, the argument for new models of care will remain theoretical. At the heart of this approach is the use of a population-based capitated contract under which providers would be expected to deliver defined outcomes for the populations they serve.
- Practices will need new skills in various areas: risk stratification of the population, quality improvement, collaborative working with other providers, greater capability in managing financial and clinical risks.
|
|
Scooped by
rob halkes
February 19, 2014 3:57 AM
|
Health Care Trends 2014 Part 1 Trend of Trends ?Just like you, I have been surprised in the past weeks of 2014 by all kind of blogs telling me what “the” trends in development of health care for 2014 will be.
Are they worthwhile to read, to watch, to be warned about? I couldn’t tell.
Some were well conceived and inspired. Others seem more like a promotional message in disguise than a valued opinion about how innovation in healthcare will continue or will be properly restrained. Who will tell? Should we bother about them? I came across all suggestions about health trends in 2014 first by @Berci (here) and Charlene Li (here). Next, I wondered what the most common perceived trends would be. I searched on health trends for 2014. See the annotated lists below. Ripe and unripe. I built my “educated guess” and now nominate the following developments as the ones that will have the highest impact on heath care developments in (the remaining of) 2014, according to me, that is: - Financial concerns. ..
- Patient Empowerment. ..
- Connected health, eHealth....
- Redefining the health industry ...
- Data Security ..
.. I suggest a different perspective: Having noticed these developments, What shouldbe the health care trend of 2014? There is a better way to approach these changes, a way that will lead us all to a constructive response to “disruption”. See part 2. What should be the trend of health care development in 2014
|
|
Scooped by
rob halkes
February 11, 2014 4:36 AM
|
When it comes to data analytics, the healthcare industry is just starting to catch up to other sectors that have been successfully using analytics for decades. "Other industries have spent a lot more time thinking about using analytics for competitive advantages and improved efficiencies," says Dr. Hughes. "But that's the first step of any 12-step program, right? You have to say you have a problem." ... Mainly through the widespread adoption and use of electronic medical records, healthcare now has what other industries from retail to banking have long enjoyed: access to large volumes of information about their customer base. "Banks have real-time trading information updated hundreds of times per second, retailers have real-time point of sale information," says Dr. Hughes. This information is currently being used to make predictions about consumer behavior that can serve as the foundation for business decisions. "A retailer is using data to understand which customer population tends to buy what products at what price sensitivity," says Dr. Hughes. "It's the same in banks; they use as much data as they can to assess your credit risk and determine which financial offerings make the most sense to you." These industries are able to use incoming data to make these projections because they have spent the past 10 to 15 years investing in the analytics infrastructure to be able to process this type of data, and developing both a team and a strategy to make the most of available information, says Dr. Hughes. "All of the Fortune 500 companies are either using data in this way or embarking on the journey make it happen," he says. This is a journey healthcare organizations have only just begun. Hospitals and health systems increasingly have access to large amounts of data about their patients, including data from EMRs, billing systems, electronic prescribing systems, health information exchanges and other similar sources. Additionally, the industry as a whole recognizes the potential in this data to provide actionable insights into population health, high-risk patient management, clinical best practices and other business insight that will become increasingly important as the industry moves toward value-based reimbursement.
|
|
Scooped by
rob halkes
February 6, 2014 4:31 AM
|
For those of us who have advocated integrated care for some time, it is premature to declare victory, says Chris Ham. The momentum behind integrated care, generated by the work of the NHS Future Forum and Norman Lamb’s appointment as Care and Support Minister, has increased during 2013. Fourteen areas that will take forward integrated care at scale and pace have been identified; the establishment of the Better Care Fund will require all areas to develop plans to integrate health and social care; and changes to the GP contract are designed to reinforce the role of GPs in co-ordinating care for older patients. Welcome as these developments are, many barriers stand in the way of translating policy aspirations into practice. While some of these barriers can only be tackled at a local level, others require changes in government policy if integrated care really is to move forward at the scale and pace demanded by current financial and service pressures. The most important changes are: ensuring that provider regulation does not get in the way of partnership workingensuring that quality regulation is not overly focused on organisational performancedeveloping payment systems that create incentives to integrate caresupporting commissioners to promote greater integration.
|
|
Scooped by
rob halkes
February 3, 2014 3:37 AM
|
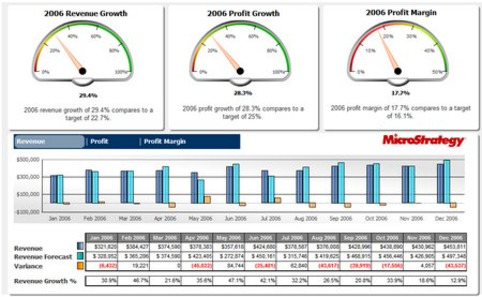
I recently interviewed Alan Kravitz, Founder and CEO of Medsys, and he offered an insight into the challenges hospitals face that I hadn’t heard before. Here’s what he said:"Expense growth is expanding faster than revenue growth for the first time in healthcare." This is really interesting to consider when you think about the billions of dollars that are being spent on EHR software. Although, I don’t think it’s the EHR expense that’s the issue. Sure, it’s now a part of the cost of running every hospital. Plus, we could certainly argue over whether it’s worth the cost and whether the EHR is overpriced. However, there’s something much more challenging at play.
Whe n you think about the political landscape for healthcare, all you hear about is the rising costs of healthcare. You also hear other things like the huge percentage of GDP that come from healthcare and how we spend so much more money than other nations around the world. With all of these things, there’s a huge drive to stop paying so much for healthcare. When you look at this trend from a hospital perspective, all you hear is that they’re going to be paying us less for doing the same thing (and some might argue for doing more). With this in mind, Alan’s quote above makes more sense. A hospital’s revenue growth is declining and that’s by design. I’m not sure most organizations are ready for this change. We’ve long heard about the potential of EHR to lower costs. Considering the pressures hospitals face today, we could really benefit from EHR living up to its potential. If not, I’m not sure where hospitals are going to cut.
|
|
Rescooped by
rob halkes
from Social Media and Healthcare
January 31, 2014 4:09 AM
|
Set goals first. If traffic, leads and sales are part of the goal, then gotta have the next focus be on content creation. Then, using social to share. Can't get much value out of social unless you're actively creating, publishing and sharing content.
Via nrip
|
|
Scooped by
rob halkes
January 31, 2014 4:06 AM
|
The ExtremeFuture of Health Care 2014from Dr. James Canton
|
|
Rescooped by
rob halkes
from Digital Pharma mktg
January 31, 2014 4:04 AM
|
|
|
Scooped by
rob halkes
January 23, 2014 10:45 AM
|
17ème édition du CEO Survey - PwC
|
|
Scooped by
rob halkes
January 22, 2014 6:08 AM
|
There are many organizations in each community whose mission can align with that of the hospital and will benefit from such a partnership. With the focus on what healthcare organizations are expected to do shifting from treating the sick to keeping people healthy comes an enormous shift in how hospitals do their work. Keeping people well requires hospitals to move much of the job from within the walls of the organization where acute care is delivered to outside the hospital into the community where prevention and early intervention and treatment are based. It's a major sea change, but hospitals don't have to go it alone. There are many organizations in each community whose mission can align with that of the hospital and will benefit from such a partnership. Working with other providers such as allied professionals and satellite community-based settings can create innovation that utilizes a wide range of resources and can more effectively support patient self-management and family-centered care.
Who will be your most important collaborators and how do you begin to build a strong partnership with them? The following five steps will help you get started. 1. Find partners providing services that advance the organization's mission and broaden its role as an essential healthcare leader .. 2. Community partners should include organizations that address the health issues represented by emergency department visits and readmissions ..
3. Look to partners that can address the social determinants of health: those factors in community residents' lives that influence their behaviors and have an impact on their health... 4. Select leaders who can move the work forward ... 5. Include evaluation metrics from the get go...
|
|
Scooped by
rob halkes
January 22, 2014 5:49 AM
|
Here are five points comparing health system strategy today versus a decade ago. Health systems used to grow by getting bigger. Now? They grow by getting better. A report from the Advisory Board (N.B. Noteworthy, see pdf at link) compares health system strategy in 2003 with that of 2013-2023. Ten years ago, health systems practiced "price-extractive growth." Growth was positioned as input and a means to advance some larger end, such as funding innovation or extending the mission. One of the key success factors under this growth strategy was expanding market share. Hospitals today and in the next 10 years will instead grow "because they're doing something right," according to the Advisory Board. Leaders must reposition growth as output rather than input, and a key determinant of growth is how a system expands covered lives. Here are five points comparing health system strategy today versus a decade ago. Key success factors for system growth
2003: Expand market share, strengthen service lines, exert pricing leverage, solidify referrals, secure physicians and increase utilization
Today: Expand covered lives, compete on outcomes, minimize total cost, assemble networks, offer convenience and expand access Performance metrics
2003: Discharges, service line share, fee-for-service revenue, pricing growth, occupancy rate, process quality
Today: Share of lives, geographic reach, risk-based revenue, share of wallet, outcomes quality, total cost of care Targets of a system's growth strategy
2003: Commercial payers, government purchasers and physicians
Today: Employers, individuals and population health managers Critical infrastructure for growth
2003: Inpatient capacity, outpatient imaging centers, ambulatory surgery centers and clinical technology
Today: Primary care capacity, care management staff and systems, health IT analytics and a post-acute care network. Competitive dynamics
2003: Service line competition, centers of excellence, referral channels, physician loyalty
Today: Comprehensive care, patient engagement, clinical quality, service quality
|
|
Scooped by
rob halkes
January 22, 2014 5:07 AM
|
HxP explores the experiences that are changing outcomes for people, for professionals, and for brands. In this report, we’ve curated some of our favorite stor At the Health Experience Project, we believe the right experience can change everything. HxP explores the experiences that are changing outcomes for people, for professionals, and for brands. In this report, we’ve curated some of our favorite stories about how brands are changing the everyday experience of healthcare. Inside, you’ll find our picks for 13 of the best experiences of 2013, ones that created new human-healthcare connections and helped more people choose better health.
|
|
Scooped by
rob halkes
January 21, 2014 10:39 AM
|
See what a master's degree can bring you. This infographic originally appeared at Ohio University's online MHA.
|
|
Scooped by
rob halkes
January 20, 2014 1:03 PM
|
Privacy experts warn there will be no way for public to work out who has their medical records or how they are using it Drug and insurance companies will from later this year be able to buy information on patients – including mental health conditions and diseases such as cancer, as well as smoking and drinking habits – once a single English database of medical data has been created. Harvested from GP and hospital records, medical data covering the entire population will be uploaded to the repository controlled by a new arms-length NHS information centre, starting in March. Never before has the entire medical history of the nation been digitised and stored in one place. Advocates say that sharing data will make medical advances easier and ultimately save lives because it will allow researchers to investigate drug side effects or the performance of hospital surgical units by tracking the impact on patients. But privacy experts warn there will be no way for the public to work out who has their medical records or to what use their data will be put. The extracted information will contain NHS numbers, date of birth, postcode, ethnicity and gender. Once live, organisations such as university research departments – but also insurers and drug companies – will be able to apply to the new Health and Social Care Information Centre (HSCIC) to gain access to the database, called care.data. If an application is approved then firms will have to pay to extract this information, which will be scrubbed of some personal identifiers but not enough to make the information completely anonymous – a process known as "pseudonymisation". However, Mark Davies, the centre's public assurance director, told the Guardian there was a "small risk" certain patients could be "re-identified" because insurers, pharmaceutical groups and other health sector companies had their own medical data that could be matched against the "pseudonymised" records. "You may be able to identify people if you had a lot of data. It depends on how people will use the data once they have it. But I think it is a small, theoretical risk," he said. (read on)
|
|
Scooped by
rob halkes
January 17, 2014 5:19 AM
|
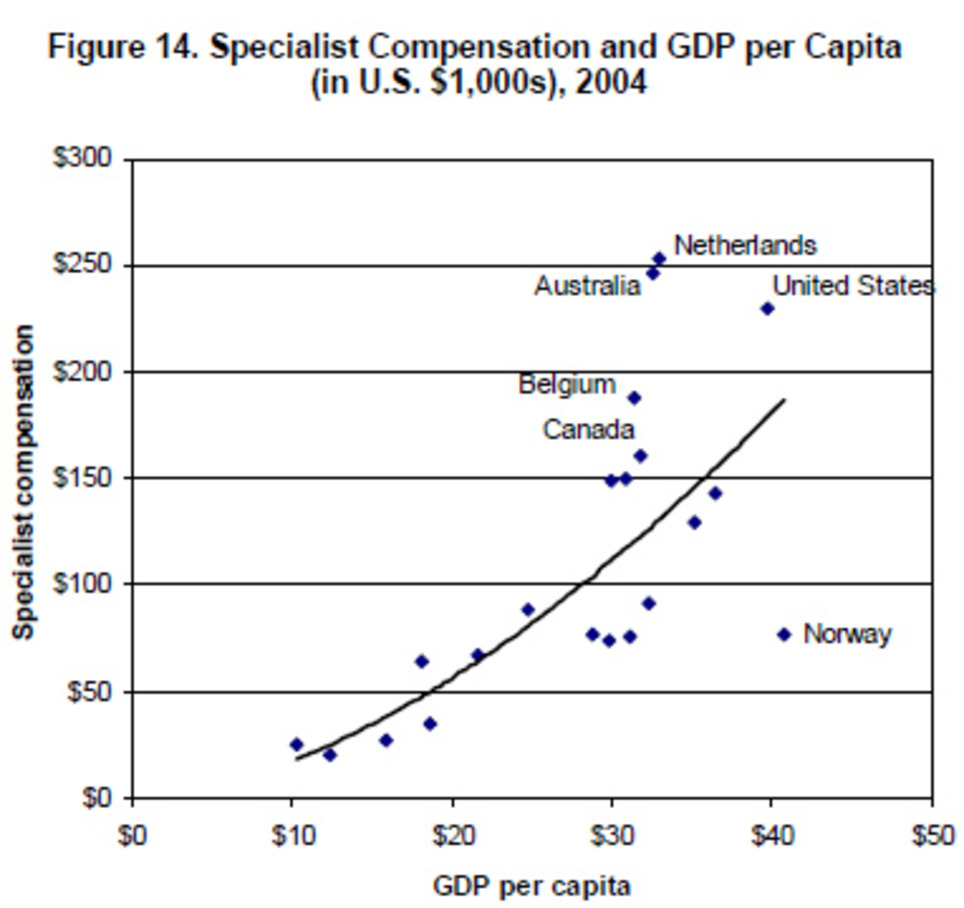
Two ways to compare physicians’ compensation in different countries. ... One way to compare cross-country data is to adjust the salaries for purchasing-power parity — that is, adjusting the numbers so that $1,000 of salary buys the same amount of goods and services in every country, providing a general sense of a physician’s standard of living in each nation. ... Another way is look at how a doctor’s salary compares to the average national income in that doctor’s country — that is, gross domestic product per capita. ... As a country’s wealth rises, so should doctors’ pay. But even accounting for this trend, the United States pays doctors more than its wealth would predict: (See graph) According to this model, the 2007 report says, “The U.S. position above the trendline indicates that specialists are paid approximately $50,000 more than would be predicted by the high U.S. GDP. General practitioners are paid roughly $30,000 more than the U.S. GDP would predict, and nurses are paid $8,000 more.” But it’s important to keep in mind, the report notes, that health care professionals in other O.E.C.D. countries pay much less (if anything) for their medical educations than do their American counterparts. In other words, doctors and nurses in the rest of the industrialized world start their medical careers with much less student loan debt compared to medical graduates in the United States. For more data on health spending in O.E.C.D. countries, go here. For a recent American-only survey on the pay of physicians with various specialties, go here.
|
|
Scooped by
rob halkes
January 14, 2014 10:04 AM
|
By Donna Roach For providers who want to involve patients in their own care and form closer ties with consumers, now might be the best time in years to implement this strategy. The Pew Research Center's Internet & American Life Project recently reported that 69% of U.S. adults track a health indicator for themselves or a loved one. The California HealthCare Foundation reported that, “Patients pay more attention and become more engaged in their health and medical care when they have easy access to their health information online.”
Although there is clear data supporting the need for providers to offer effective and user-engaging patient portals, many systems launched to date have fallen short of meeting patients' needs. Providers have made a commitment to discovering why this is the case, driven by pressures to meet the expectations of patients and communities.
A patient portal is a secure online website that offers consumers convenient 24-hour access to personal health information and medical records through an Internet connection. A portal should be a starting point for other sites, provide the capability to usher in new applications and technology and streamline processes. A patient portal should also engage the users and encourage them to regularly access their information.
So why aren't patient portals more common?
Other consumer-friendly portals provide ready examples of how to facilitate interactions and engage users. For example, Pinterest is the fastest-growing social network, accessed by 15% of American Internet users. Pinterest is a pinboard-style photo-sharing website that enables users to create and manage their own image collections or events, interests and hobbies. Each “pin” posted to the site serves as a portal into a personal web collection or other themed sites.
On the other hand, Facebook and Twitter provide more up-to-date content and real news information than most standard news sites. And ESPN.com provides access to a variety of sports portals for up-to-date content. These sites have one thing in common—users interact with the sites many times a day, returning multiple times to access new content.
This type of engagement should be the ultimate goal for patient portals.
To achieve that goal, patient portals must include secure messaging linking patients and the provider, prescription refills, lab results and online bill payment. In my organization, we offer a patient portal that is directly integrated with the enterprise electronic health record. Additional features include appointment requests and verification; demographic information updates; laboratory results and patient education materials; clinical record summaries; continuity of care document downloads; discharge information and online bill payment.
We introduced the portal in March 2013, and it now has 13,000 active users. That growth was driven by efforts to increase awareness of the portal's benefits among our patients and community, and their realization that the portal's benefits go far beyond general convenience. The portal is helping to alleviate follow-up phone calls to physician offices. In the past year, we also introduced the portal to inpatients, offering them access to discharge information and follow-up patient care instructions. As the portal evolves, we're planning improvements and upgrades.
The portal also has served as a successful measurement for meaningful use Stage 1. Stage 2 also sets objectives for patient engagement for which portals could prove effective. Overall, the most significant benefit of the portal has been the opportunity to offer an accessible, effective engagement tool to patients and the community.
Our patient portal is much more than just an online tool; it supports a strategy focused on enhancing patient engagement within our community and with our providers. As the industry becomes more focused on ambulatory care, the portal is another way to strengthen our ambulatory presence and reach more individuals beyond hospital walls. The patient portal can also be an efficient and effective method of communicating with patients outside of the office. The most pronounced portal benefit, however, is the improvement in healthcare quality it encourages, stemming from patients' active engagement in their health and healthcare.
|
|
Scooped by
rob halkes
January 13, 2014 3:24 AM
|
Dr. Pierre Theodore of UC San Francisco has completed a three-month trial using Google Glass during surgery. For a little over three months now, Dr. Pierre Theodore, a cardiothoracic surgeon, has been using Google Glass in the operating room. Although he's tapped the functionality during procedures on just 10 patients, for various cancer mass removals, fluid removal, and a lung restoration, Theodore (who we first wrote about in August) may have more experience using Glass in a serious medical setting than any other doctor in the world. His conclusion so far: the technology is indeed useful in the operating room as an adjunct device in delivering necessary information, but it still has miles to go as a product.... Read on!
|
|
Scooped by
rob halkes
January 7, 2014 8:16 AM
|
By Craig M. Lilly, MD; John M. McLaughlin, PhD, MSPH; Huifang Zhao; Stephen P. Baker, MScPH, (abd); Shawn Cody, RN, MSN, MBA; Richard S. Irwin, MD; on behalf of for the UMass Memorial Critical Care Operations Group Abstract Background Few studies have evaluated both the overall effect of intensive care unit (ICU) telemedicine programs and the effect of individual components of the intervention on clinical outcomes. Methods The effects of non-randomized ICU telemedicine interventions on crude and adjusted mortality and length of stay (LOS) were measured. Additionally, individual intervention components related to process and setting of care, were evaluated for their association with mortality and LOS. Results Overall, 118,990 (11,558 control; 107,432 intervention) adult patients from 56 ICUs in 32 hospitals from 19 US health care systems were included. After statistical adjustment, hospital (HR=0.84, 95%CI: 0.78-0.89, p<.001) and ICU (HR=0.74, 95%CI: 0.68-0.79, p<.001) mortality in the ICU telemedicine intervention group was significantly better than that of controls. Moreover, adjusted hospital LOS was reduced, on average, by 0.5 (95%CI: 0.4-0.5), 1.0 (95%CI: 0.7-1.3), and 3.6 (95%CI: 2.3-4.8) days, and adjusted ICU LOS was reduced by 1.1 (95%CI: 0.8-1.4), 2.5 (95%CI: 1.6-3.4), and 4.5 (95%CI: 1.5-7.2) days among those who stayed in the ICU for ≥7, ≥14, and ≥30 days, respectively. Individual components of the interventions that were associated with lower mortality and/or reduced LOS included: i) intensivist case review within 1 hour of admission, ii) timely use of performance data, iii) adherence to ICU best practices, and iv) quicker alert response times. Conclusions ICU telemedicine interventions, specifically interventions that increase early intensivist case involvement, improve adherence to ICU best practices, reduce response times to alarms, and encourage the use of performance data were associated with lower mortality and LOS.
|
|
Scooped by
rob halkes
January 6, 2014 11:21 AM
|
Google Glass in Surgery, by GoogleGlassSurgeon: News on use of Google Glass in Surgery and medical apps for GoogleGlass
|
|
Scooped by
rob halkes
November 10, 2013 12:56 PM
|
The income statements of hospitals have been ailing. The cure? Serious attention to operating efficiency. A McKinsey Quarterly article.
|
|
Rescooped by
rob halkes
from New pharma
November 8, 2013 5:46 AM
|
As the health service grapples with the need to provide quality care while containing spiralling patient care costs (something all stakeholders will need to do for decades to come), the ability to manage care in a holistic, safe and cost effective way is a priority for commissioners. Choosing the best healthcare partner to deliver these often complex and detailed healthcare requirements is high on the agenda for many commissioners and with the recent changes to NHS commissioning and the publication of the Homecare Medicines Review guidelines, this task has become even more important to get right first time round. So what can you do to ensure the right partnerships are formed that best meet your individual service objective needs? First of all, the healthcare partner should offer a broad and integrated range of services such as medicines distribution/logistics, clinical homecare, medicines support, dispensing services, medicine preparation and clinical trial support. Not only does provision of these cohesive services avoid the need for other external partners and contracts, but it also creates the flexibility to add-on future services as end-to-end patient healthcare needs develop and expand. In addition, this fully integrated approach has a greater potential to lead to service efficiencies, flexible service delivery and improved patient care. .. The healthcare partner must help patients make better use of the medicines and therapies they are prescribed and by doing so, the NHS can be supported to deliver the demands of the Government's QIPP (Quality, Innovation, Productivity and Prevention) agenda .. .. Most importantly, a partner should be able to demonstrate a strong track record of patient-centric care that supports patients throughout their care journey... An aspect which is perhaps given less weight is the existence of shared values and complementary multi-disciplinary expertise between stakeholder organisations. In my opinion, evidence of this is critical to engender mutual trust and respect between both organisations, as no doubt the ability for co-operative working will be tested under the current challenging and changing healthcare environment. Ultimately, the true measure of success will be the strength of the relationship between the healthcare provider and partner as they work together in the pursuit of mutual goals to deliver the best possible care for their patients.
|
|
Scooped by
rob halkes
November 7, 2013 1:46 PM
|
A team of British researchers is warning governments and health care organizations around the world not to fall for the myths and hype surrounding medical tourism. With the promise of a lucrative market and huge global market opportunities, the appeal of medical tourism is hard to miss. But researchers from London, York, Sheffield and Birmingham, UK, challenge the view that there is an ever-growing number of people prepared to travel across national borders to receive medical treatment. .. Medical tourists are not to be confused with health tourists, who may not always intend to pay for their treatments. The report, published by the Organisation for Economic Co-operation and Development (OECD)[ see here: http://www.oecd.org/els/health-systems/48723982.pdf ], looks at the flow of medical tourists between countries and the interaction between the demand for, and supply of, these services. .. Price is not the only determining factor when it comes to choosing a destination. The authors argue that in terms of medical tourism, there is not necessarily a level playing field, and they challenge the view of open and global markets. They say it is not as simple as building facilities and expecting patients to come... The study also points out that there is currently no overarching legal or ethical strategy for medical tourism, and the researchers call for more information and understanding before even considering what regulations are needed. But as to whether medical tourism is a good or bad thing, the researchers decline to call. The report concludes: "On balance there is a pressing need to explore further as to whether medical tourism is virus, symptom, or cure."
|
|
Scooped by
rob halkes
November 7, 2013 9:03 AM
|
Today's talk involves examining the boomerag effect. Discussing financial implications for Telehealth. Discussing Vidant Health’s Telehealth Program and outcomes.chronic illness and the "Boomerang Effect" :
Mr. Doe's Hospital Admission requires the 81 y.o : CVD,HF, DM, Arthritis. Exacerbation of heart failure consists not following his diet, not talking all of his medications, not keeping PCP visits and low engagement level. 8 HF ER visits and 6 hospitalizations less than 12 mos. Mr. Doe prepares for discharge told he will be d/c home tomorrow, PCP not alerted that Mr. doe was hospitalized, given new prescriptions and told to schedule a PCP appt. in the next month.
Patient education requires smoking, Diabetes care, Nutrition and cooking advice to him and his wife. Must take BP meds even if he feels fine and How to take his diuretics. The boomerang effect. Patient issues. Don’t understand their medications. Don’t understand how to follow prescribed diet, Can’t afford their medications, Can’t afford foods to follow their diet and Low engagement level. The hospitalissues are Focus: inside walls of the hospital, Post d/c service focus: HH & LTC, Incorrect or absent medication reconciliation, Extremely limited system of care transitions, Brief & fragmented patient education, PCP not contacted during hospitalization, Fragmented communication between clinics/specialists/hospital, Dictate to patients vs. engage them in their care. vidant health\92s mission: To enhance the q ...Please navigate Paper pages for more details.
|
|
Scooped by
rob halkes
November 7, 2013 7:42 AM
|
Navigating Health Reform, the Future of Health Care, and Telemedicine’s Expanding Role. The Agenda include Quick overview of the Affordable Care Act, What’s popular, what’s controversial, The promise and key disconnects, Costs, Workforce a dequacy The States: Medicaid Expansion and Insurance Exchanges, Stay tuned, What we don’t know, Critical disconnects, What is happening in spite of reform andTelemedicine’s expanding role. What is good a bout the health care delivery system? the John’s List consists Robust medical community, well represented by specialties. Strong & dedicated allied health workforce. Best education system in the world across all disciplines. Cutting edge technologies & pharmaceuticals. Strong research basis. Social safety net. Modern physical plant. Improving transparency & accountability Improving quality & safety and Major economic engine, frequently largest employer.What is not good about the health care delivery system? the Patient Protection and Affordable Care Act (PPACA): Signed into Law March 23, 2010 include Most comprehensive change in healthcare finance since 1964 Medicare & Medicaid legislation, Reforms the actuarial financing model for health services in the United States, Improves access to care for most citizens and reduces the number of uninsured, Reins in unpopular insurance industry practices, Increases quality and safety of health care, Improves transparencyof health and insurance information, Creates Health Insurance ...Please navigate Paper pages for more details.
|



































Here's the research demonstrating value of ICU telemedicine reengineering of adult critical care.