Your new post is loading...
Your new post is loading...

|
Scooped by
Gilbert C FAURE
December 27, 2023 4:15 AM
|
Scientific evidence regularly guides policy decisions1, with behavioural science increasingly part of this process2. In April 2020, an influential paper3 proposed 19 policy recommendations (‘claims’) detailing how evidence from behavioural science could contribute to efforts to reduce impacts and end the COVID-19 pandemic. Here we assess 747 pandemic-related research articles that empirically investigated those claims. We report the scale of evidence and whether evidence supports them to indicate applicability for policymaking. Two independent teams, involving 72 reviewers, found evidence for 18 of 19 claims, with both teams finding evidence supporting 16 (89%) of those 18 claims. The strongest evidence supported claims that anticipated culture, polarization and misinformation would be associated with policy effectiveness. Claims suggesting trusted leaders and positive social norms increased adherence to behavioural interventions also had strong empirical support, as did appealing to social consensus or bipartisan agreement. Targeted language in messaging yielded mixed effects and there were no effects for highlighting individual benefits or protecting others. No available evidence existed to assess any distinct differences in effects between using the terms ‘physical distancing’ and ‘social distancing’. Analysis of 463 papers containing data showed generally large samples; 418 involved human participants with a mean of 16,848 (median of 1,699). That statistical power underscored improved suitability of behavioural science research for informing policy decisions. Furthermore, by implementing a standardized approach to evidence selection and synthesis, we amplify broader implications for advancing scientific evidence in policy formulation and prioritization. Evaluation of evidence generated to test 19 proposed policy recommendations and guidance for the future.
|
|
Scooped by
Gilbert C FAURE
December 4, 2023 4:26 AM
|
On 5 May 2023, the World Health Organization (WHO) officially declared the end of the coronavirus disease-19 (or COVID-19) pandemic. Even before the official announcement from the WHO, signs of recovery from the pandemic started appearing, especially after rapid worldwide vaccination.
|
|
Scooped by
Gilbert C FAURE
August 29, 2023 7:55 AM
|
Cochrane Database of Systematic Reviews Review - Intervention Collapse all Expand all Résumé scientifique available in Contexte Différentes formes de vaccins ont été développées pour prévenir le virus SARS‐CoV‐2 et la COVID‐19 qui en découle. Plusieurs d'entre elles sont largement utilisées dans le monde. Objectifs Évaluer l'efficacité et la tolérance des vaccins contre la COVID‐19 (en tant que série complète de primovaccination ou dose de rappel) contre le SARS‐CoV‐2. Stratégie de recherche documentaire Nous avons effectué des recherches dans le registre Cochrane des études sur la COVID‐19 et dans la plateforme COVID‐19 L·OVE (dernière date de recherche le 5 novembre 2021). Nous avons également effectué des recherches sur le Système d'enregistrement international des essais cliniques (ICTRP) de l’OMS, sur les sites Web des organismes de réglementation et sur Retraction Watch. Critères de sélection Nous avons inclus des essais contrôlés randomisés (ECR) comparant les vaccins contre la COVID‐19 à un placebo, à l'absence de vaccin, à d'autres vaccins actifs ou à d'autres schémas vaccinaux. Recueil et analyse des données Nous avons utilisé les méthodes standard de Cochrane. Nous avons utilisé le système GRADE pour évaluer le niveau de confiance des données probantes pour tous les critères de jugement, à l'exception de l'immunogénicité. Nous avons synthétisé les données pour chaque vaccin séparément et présenté des estimations globales de l'effet avec des intervalles de confiance (IC) à 95 %. Résultats principaux Nous avons inclus et analysé 41 ECR évaluant 12 vaccins différents, y compris les schémas vaccinaux homologues et hétérologues et l'effet des doses de rappel. Trente‐deux ECR étaient multicentriques et cinq étaient multinationaux. La taille des échantillons des ECR était de 60 à 44 325 participants. Les participants étaient âgés: 18 ans ou plus dans 36 ECR ; 12 ans ou plus dans un ECR ; 12 à 17 ans dans deux ECR ; et 3 à 17 ans dans deux ECR. Vingt‐neuf ECR ont fourni des résultats pour des personnes âgées de plus de 60 ans, et trois ECR ont inclus des patients immunodéprimés. Aucun essai n'a inclus des femmes enceintes. Seize ECR avaient un suivi de deux mois ou moins, 20 ECR avaient un suivi de deux à six mois et cinq ECR avaient un suivi de plus de six à douze mois ou moins. Dix‐huit rapports étaient basés sur des analyses intérimaires planifiées à l'avance. Le risque global de biais était faible pour tous les critères de jugement dans huit ECR, tandis que 33 présentaient des problèmes pour au moins un critère de jugement. Nous avons identifié 343 ECR enregistrés dont les résultats ne sont pas encore disponibles. Ce résumé rapporte les résultats pour les critères de jugement critiques de la COVID‐19 symptomatique et confirmée, la forme sévère et critique de la COVID‐19, et des événements indésirables graves uniquement pour les 10 vaccins approuvés par l'OMS. Pour les autres critères de jugement et les vaccins, voir le texte principal. Les données probantes relatives à la mortalité étaient généralement éparses et d'un niveau de confiance faible ou très faible pour tous les vaccins approuvés par l'OMS, à l'exception du vaccin AD26.COV2.S (Janssen), qui réduit probablement le risque de mortalité toutes causes confondues (risque relatif (RR) 0,25, IC à 95 % 0,09 à 0,67 ; 1 ECR, 43 783 participants ; données probantes d’un niveau de confiance élevé). COVID‐19 symptomatique et confirmée Des données probantes d’un niveau de confiance élevé ont révélé que le BNT162b2 (BioNtech/Fosun Pharma/Pfizer), le mRNA‐1273 (ModernaTx), le ChAdOx1 (Oxford/AstraZeneca), l’Ad26.COV2.S, le BBIBP‐CorV (Sinopharm‐Beijing) et le BBV152 (Bharat Biotect) réduisent l'incidence de la COVID‐19 symptomatique par rapport au placebo (efficacité vaccinale (EV) : BNT162b2: 97,84 %, IC à 95 % 44,25 % à 99,92 % ; 2 ECR, 44 077 participants ; mRNA‐1273 : 93,20 %, IC à 95 % 91,06 % à 94,83 % ; 2 ECR, 31 632 participants ; ChAdOx1 : 70,23 %, IC à 95 % 62,10 % à 76,62 % ; 2 ECR, 43 390 participants ; Ad26.COV2.S : 66,90 %, IC à 95 % 59,10 % à 73,40 % ; 1 ECR, 39 058 participants ; BBIBP‐CorV : 78,10%, IC à 95 % 64,80 % à 86,30 % ; 1 ECR, 25 463 participants ; BBV152: 77,80 %, IC à 95 % 65,20 % à 86,40 % ; 1 ECR, 16 973 participants). Des données probantes d’un niveau de confiance modéré indiquent que le NVX‐CoV2373 (Novavax) réduit probablement l'incidence de la COVID‐19 symptomatique par rapport au placebo (EV 82,91 %, IC à 95 % 50,49 % à 94,10 % ; 3 ECR, 42 175 participants). Il existe des données probantes d’un niveau de confiance faible pour CoronaVac (Sinovac) pour ce critère de jugement (EV 69,81 %, IC à 95 % 12,27 % à 89,61 % ; 2 ECR, 19 852 participants). Forme sévère ou critique de la COVID‐19 Des données probantes d’un niveau de confiance élevé ont révélé que le BNT162b2, le mRNA‐1273, l’Ad26.COV2.S et le BBV152 entraînent une réduction importante de l'incidence de la forme sévère ou critique de la COVID‐19 par rapport au placebo (EV : BNT162b2: 95,70 %, IC à 95 % 73,90 % à 99,90 % ; 1 ECR, 46 077 participants ; mRNA‐1273 : 98,20 %, IC à 95 % 92,80 % à 99,60 % ; 1 ECR, 28 451 participants ; AD26.COV2.S : 76,30 %, IC à 95 % 57,90 % à 87,50 % ; 1 ECR, 39 058 participants ; BBV152: 93,40 %, IC à 95 % 57,10 % à 99,80 % ; 1 ECR, 16 976 participants). Des données probantes d’un niveau de confiance modéré ont montré que le NVX‐CoV2373 réduit probablement l'incidence de la forme sévère ou critique de la COVID‐19 (EV 100,00 %, IC à 95 % 86,99 % à 100,00 % ; 1 ECR, 25 452 participants). Deux essais ont rapporté une efficacité élevée de CoronaVac pour la forme sévère ou critique de la COVID‐19 avec des IC larges, mais ces résultats n'ont pas pu être regroupés. Événements indésirables graves (EIG) Le mRNA‐1273, le ChAdOx1 (Oxford‐AstraZeneca)/SII‐ChAdOx1 (Serum Institute of India), l’Ad26.COV2.S et le BBV152 entraînent probablement peu ou pas de différence dans les EIG par rapport au placebo (RR : mRNA‐1273 : 0,92, IC à 95 % 0,78 à 1,08 ; 2 ECR, 34 072 participants ; ChAdOx1/SII‐ChAdOx1 : 0,88, IC à 95 % 0,72 à 1,07 ; 7 ECR, 58 182 participants ; Ad26.COV2.S : 0,92, IC à 95 % 0,69 à 1,22 ; 1 ECR, 43 783 participants) ; BBV152: 0,65, IC à 95 % 0,43 à 0,97 ; 1 ECR, 25 928 participants). Dans chacun de ces résultats, la différence absolue probable des effets était inférieure à 5/1000 participants. Les données probantes des EIG sont incertaines pour le BNT162b2, le CoronaVac, le BBIBP‐CorV et le NVX‐CoV2373 par rapport au placebo (RR : BNT162b2: 1,30, IC à 95 % 0,55 à 3,07 ; 2 ECR, 46 107 participants ; CoronaVac : 0,97, IC à 95 % 0,62 à 1,51 ; 4 ECR, 23 139 participants ; BBIBP‐CorV : 0,76, IC à 95 % 0,54 à 1,06 ; 1 ECR, 26 924 participants ; NVX‐CoV2373: 0,92, IC à 95 % 0,74 à 1,14 ; 4 ECR, 38 802 participants). Pour l'évaluation des schémas hétérologues, des doses de rappel et de l'efficacité contre les variants préoccupants, voir le texte principal de la revue. Conclusions des auteurs Par rapport au placebo, la plupart des vaccins réduisent, ou réduisent probablement, la proportion de participants présentant une COVID‐19 symptomatique et confirmée, et pour certains, il existe des données probantes d’un niveau de confiance élevé indiquant qu'ils réduisent la forme sévère ou critique de la maladie. Il y a probablement peu ou pas de différence entre la plupart des vaccins et le placebo en ce qui concerne les événements indésirables graves. Plus de 300 ECR enregistrés évaluent l'efficacité des vaccins contre la COVID‐19, et cette revue est régulièrement mise à jour sur la plateforme COVID‐NMA(covid-nma.com). Implications pour la pratique En raison des critères d’exclusions des essais, ces résultats ne peuvent être généralisés aux femmes enceintes, aux personnes ayant des antécédents d'infection par le SARS‐CoV‐2 ou aux personnes immunodéprimées. La plupart des essais avaient un suivi court et ont été menés avant l'émergence des variants préoccupants. Implications pour la recherche Les recherches futures devraient évaluer l'effet à long terme des vaccins, comparer différents vaccins et schémas vaccinaux, évaluer l'efficacité et la tolérance des vaccins dans des populations spécifiques, et inclure des critères de jugement tels que la prévention de la COVID‐19 de longue durée. Il est également essentiel d'évaluer en permanence l'efficacité des vaccins et leur efficacité contre les nouveaux variants préoccupants. PICOs Population Intervention Comparison Outcome The PICO model is widely used and taught in evidence-based health care as a strategy for formulating questions and search strategies and for characterizing clinical studies or meta-analyses. PICO stands for four different potential components of a clinical question: Patient, Population or Problem; Intervention; Comparison; Outcome. See more on using PICO in the Cochrane Handbook. Résumé simplifié available in Quels sont les bénéfices et les risques des vaccins dans la prévention de la COVID‐19 ? Principaux messages ‐ La plupart des vaccins réduisent, ou réduisent probablement, le nombre de personnes qui contractent la COVID‐19 et la forme sévère de la COVID‐19. ‐ De nombreux vaccins sont susceptibles d'augmenter le nombre de personnes présentant des manifestations telles que fièvre ou maux de tête par rapport à un placebo (vaccin factice ne contenant aucun médicament mais ayant l'apparence du vaccin testé). Ceci est attendu car ces événements sont principalement dus à la réponse de l'organisme au vaccin ; ils sont généralement légers et de courte durée. ‐ De nombreux vaccins présentent peu ou pas de différence dans l'incidence des événements indésirables graves par rapport au placebo. ‐ Les données probantes sont insuffisantes pour déterminer s'il y avait une différence entre le vaccin et le placebo en termes de décès, car le nombre de décès était faible dans les essais. ‐ La plupart des essais ont évalué l'efficacité du vaccin sur une courte période, et n'ont pas évalué l'efficacité contre les variants préoccupants de la COVID‐19. Qu'est‐ce que le SARS‐CoV‐2 et la COVID‐19 ? Le SARS‐CoV‐2 (coronavirus 2 du syndrome respiratoire aigu sévère) est le virus à l'origine de la maladie à coronavirus 2 (COVID‐19). Les personnes infectées par le SARS‐CoV‐2 ne développent pas toutes les symptômes de la COVID‐19. Les symptômes peuvent être légers (fièvre et maux de tête, par exemple) ou menacer le pronostic vital (difficultés respiratoires, par exemple), voire entraîner la mort. Comment les vaccins préviennent‐ils la COVID‐19 ? Bien que les vaccins fonctionnent de manière légèrement différente, ils préparent tous le système immunitaire de l'organisme à empêcher les personnes d'être infectées par le SARS‐CoV‐2 ou, si elles le sont, à prévenir une forme sévère de la maladie. Que voulions‐nous découvrir ? Nous avons voulu savoir dans quelle mesure chaque vaccin est efficace pour réduire l'infection par le SARS‐CoV‐2, la COVID‐19 avec symptômes, la forme sévère de la COVID‐19 et le nombre total de décès (y compris tous les décès, pas seulement ceux liés à la COVID‐19). Nous voulions connaître les événements indésirables graves pouvant nécessiter une hospitalisation, mettre la vie en danger, ou les deux ; les événements de réactogénicité systémique (réactions immédiates à court terme aux vaccins principalement dues à des réponses immunologiques ; par exemple, fièvre, maux de tête, douleurs corporelles, fatigue) ; et tous les événements indésirables (qui comprennent les événements indésirables non graves). Qu'avons‐nous fait ? Nous avons recherché les études qui ont examiné tout vaccin contre la COVID‐19 comparé à un placebo, à l'absence de vaccin ou à un autre vaccin contre la COVID‐19. Nous n'avons retenu que les essais randomisés (un plan d'étude qui fournit les données probantes les plus solides car il évalue les interventions dans des conditions idéales parmi des participants assignés par hasard à l'un des deux groupes ou plus). Nous avons comparé et résumé les résultats des études, et évalué notre confiance dans les données probantes en fonction de facteurs tels que la manière dont l'étude a été menée. Qu'avons‐nous trouvé ? Nous avons trouvé 41 études mondiales impliquant 433 838 personnes et évaluant 12 vaccins différents. Trente‐cinq études n'ont inclus que des personnes en bonne santé qui n'avaient jamais eu la COVID‐19. Trente‐six études ne comprenaient que des adultes, deux que des adolescents, deux des enfants et des adolescents, et une comprenait des adolescents et des adultes. Trois ont étudié des personnes au système immunitaire affaibli, et aucune n'a étudié des femmes enceintes. Dans la plupart des cas, les résultats ont été évalués moins de six mois après la primovaccination. La plupart ont bénéficié d'un cofinancement de la part d'institutions universitaires et de sociétés pharmaceutiques. La plupart des études ont comparé un vaccin contre la COVID‐19 avec un placebo. Cinq d'entre eux ont évalué le mélange des vaccins pour la dose de rappel. Principaux résultats Nous présentons ci‐dessous les résultats pour trois critères de jugement principaux et pour dix vaccins approuvés par l'Organisation mondiale de la santé (OMS) (pour les autres critères de jugement et vaccins, voir le texte principal). Les données probantes concernant les décès sont insuffisantes entre les vaccins et le placebo (principalement car le nombre de décès était faible), à l'exception du vaccin Janssen, qui réduit probablement le risque de décès toutes causes confondues. Personnes présentant des symptômes Les vaccins Pfizer, Moderna, AstraZeneca, Sinopharm‐Beijing et Bharat entraînent une forte réduction du nombre de personnes présentant des symptômes de la COVID‐19. Le vaccin de Janssen réduit le nombre de personnes présentant des symptômes de la COVID‐19. Le vaccin Novavax a probablement permis de réduire considérablement le nombre de personnes présentant des symptômes de la COVID‐19. Les données probantes sont insuffisantes pour déterminer si le vaccin CoronaVac affecte le nombre de personnes présentant des symptômes de la COVID‐19 car les résultats diffèrent entre les deux études (l'une ne concernait que les travailleurs de la santé avec un risque d'exposition plus élevé). Forme sévère de la maladie Les vaccins Pfizer, Moderna, Janssen et Bharat permettent de réduire considérablement le nombre de personnes atteintes d'une forme sévère de la maladie. Les données probantes concernant le vaccin CoronaVac sur la forme sévère de la maladie sont insuffisantes car les résultats diffèrent entre les deux études (l'une ne concernait que les travailleurs de la santé, avec un risque d'exposition plus élevé). Événements indésirables graves Pour les vaccins Pfizer, CoronaVac, Sinopharm‐Beijing et Novavax, les données probantes sont insuffisantes pour déterminer s'il y avait une différence entre le vaccin et le placebo, principalement car le nombre d'événements indésirables graves était faible. Les vaccins Moderna, AstraZeneca, Janssen et Bharat n'entraînent probablement pas ou peu de différence dans le nombre d'événements indésirables graves. Quelles sont les limites des données probantes ? La plupart des études ont évalué le vaccin pendant une courte période après l'injection, et on ne sait pas si et comment la protection vaccinale s'estompe avec le temps. En raison des critères d'exclusion des essais des vaccins contre la COVID‐19, les résultats ne peuvent être généralisés aux femmes enceintes, aux personnes ayant des antécédents d'infection par le SARS‐CoV‐2 ou aux personnes dont le système immunitaire est affaibli. Des recherches supplémentaires sont nécessaires pour comparer les vaccins et les schémas vaccinaux, ainsi que l'efficacité et la sécurité dans des populations et des critères de jugement spécifiques (par exemple, la prévention de la COVID‐19 de longue durée). En outre, la plupart des études ont été menées avant l'émergence des variants préoccupants. Ces données probantes sont‐elles à jour ? Les données probantes sont à jour jusqu'en novembre 2021. Il s'agit d'une revue systématique dynamique. Nos résultats sont disponibles et mis à jour toutes les deux semaines sur la plateforme COVID‐NMA à l'adresse covid‐nma.com (disponibles en anglais). Authors' conclusions Implications for practice Several COVID‐19 vaccines are highly effective or probably highly effective in preventing SARS‐CoV‐2 infection, symptomatic COVID‐19 and severe or critical COVID‐19. There is moderate‐ to high‐certainty evidence that most vaccine candidates increased the risk of systemic reactogenicity events (e.g. fever). Evidence related to any adverse event was mainly uncertain. There is moderate‐ to high‐certainty evidence that there is probably no difference between mRNA‐1273, CVnCoV, ChAdOx1, Ad26.COV2.S, Gam‐COVID‐Vac, WIBP‐CorV and BBIBP‐CorV and placebo in terms of serious adverse events. Evidence was uncertain and very uncertain for serious adverse events for other vaccines and for all‐cause mortality for most vaccines, mainly because of the low number of events. In addition, as most RCTs only followed up participants for 2 months after full vaccination, all reports are related to short‐term impacts of the vaccine. Results cannot easily be generalized to pregnant women and immunocompromized individuals; more evidence is needed to elucidate the degree of additional protection conferred by COVID‐19 vaccines in these populations. Finally, the advent of variants of concern has highlighted the need for further research on each of the vaccine’s capacity to limit infection, disease, and death in regard to specific variants of concern. Implications for research Three hundred and forty‐four RCTs are currently registered, of which 10 are completed. The findings from these trials will contribute to the body of evidence on efficacy and safety outcomes. The findings of this review will be updated as soon as new data are available on the COVID‐NMA platform. Since the efficacy of vaccines is well established at this point, the ethics of RCT designs using a placebo as the comparison group should be questioned, and active comparators should be considered. With the notable impact of variants of concern on vaccine efficacy, it is crucial that variant type is assessed in clinical trials and reported for future meta‐analyses to assess vaccine efficacy on considerably different variants. As a non‐negligible global population has been infected by SARS‐CoV‐2, robust evidence‐based vaccination schemes are also required. Finally, considering the rapidly changing situation (in terms of variants, policies, etc.) and the increasing and important heterogeneity in the population in terms of combinations of vaccines received, history of SARS‐CoV‐2 infection (and by which variant), type of booster vaccine received, and predominant variants at the time of data collection, RCTs might become increasingly difficult to conduct in such a rapidly‐changing context and large population‐based observational studies could provide relevant information. Summary of findings Open in table viewerSummary of findings 1. BNT162b2 – Pfizer/BioNTech + Fosun Pharma compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants Certainty of the evidence(GRADE) Comments Risk with placebo Risk with BNT162b2 Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19b 3923 per 100,000 85 per 100,000(3 to 2187) VE 97.84 (44.25 to 99.92) 44,077(2 RCTs)c ⊕⊕⊕⊕Highd — Severe or critical COVID‐19e 100 per 100,000 4 per 100,000(0 to 26) VE 95.70(73.90 to 99.90) 46,077(1 RCT)f ⊕⊕⊕⊕High — All‐cause mortalityg 64 per 100,000 68 per 100,000(33 to 142) RR 1.07(0.52 to 2.22) 43,847(1 RCT)f ⊕⊕⊖⊖Lowh 2 additional studies (Frenck 2021 (adolescents aged 12–15 years); Walsh 2020 (adults aged 18–85 years)) reported this outcome in 2302 participants (1131 versus 1129 participants and 24 versus 18 participants in the BNT162b2 versus placebo groups, respectively). There were no events in either group and the trials did not contribute to the effect estimate. Systemic reactogenicity events Outcome not yet measured or reported Any adverse eventi Outcome not pooled due to considerable heterogeneity (I² = 90%) between included studies: Thomas 2021 (≥ 16 years): RR 2.17, 95% CI 2.09 to 2.26; n = 43,847; Frenck 2021 (12–15 years): RR 1.01, 95% CI 0.73 to 1.41; n = 2260; Walsh 2020 (≥ 18 years): RR 1.50, 95% CI 0.53 to 4.21; n = 42 46,149(3 RCTs)j ⊕⊕⊖⊖Lowk — Serious adverse eventsi 508 per 100,000 660 per 100,000(279 to 1558) RR 1.30(0.55 to 3.07) 46,107(2 RCTs)c ⊕⊕⊖⊖Lowl,m 1 additional trial (Walsh 2020 (adults aged 18–85 years)) reported this outcome in 42 participants (24 BNT162b2 versus 18 placebo). There were no events in either group and the trial did not contribute to the effect estimate. Local reactogenicity events Outcome not yet measured or reported *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019;CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 3 May 2022bFollow‐up: from 7 days following the second dose to 1.81 months and six months.cBioNTech/Fosun Pharma/Pfizer: Thomas 2021 (adolescents and adults aged from 16 years); Frenck 2021 (adolescents aged 12–15 years)dDespite some concerns with deviations from intervention, not downgraded for risk of bias.eFollow‐up: from seven days following the second dose to six months.fBioNTech/Fosun Pharma/Pfizer: Thomas 2021 (adolescents and adults aged from 16 years)gFollow‐up: six monthshImprecision: downgraded two levels due to small number of events observed and a wide CIs that encompasses a potential benefit and a potential harm with the intervention.iFollow‐up: 1.7 monthsjBioNTech/Fosun Pharma/Pfizer: Thomas 2021 (adolescents and adults aged from 16 years); Frenck 2021 (adolescents aged 12–15 years); Walsh 2020 (adults aged 18–85 years)kInconsistency: downgraded two levels (I² = 90%)lInconsistency: downgraded one level (I² = 76%)mImprecision: downgraded one level due to wide CIs consistent with the possibility of benefit and the possibility of harm. This outcome was not downgraded an additional level for imprecision because it was downgraded one level for inconsistency, which is related to and would have contributed to the severity of the imprecision. Open in table viewerSummary of findings 2. mRNA‐1273 – ModernaTX compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with placebo Risk with mRNA‐1273 Confirmed SARS‐CoV‐2 infectionb 8957 per 100,000 2394 per 100,000(997 to 5749) VE 73.27(35.82 to 88.87) 31,632(2 RCTs)c ⨁⨁⨁◯Moderated,e Substantial heterogeneity (I² = 66%) between included studies: Ali 2021 (adolescents aged 12–17 years, median 2.3 months' follow‐up): VE 55.7% (95% CI 16.8 to 76.4), n = 3181; El Sahly 2021 (adults aged 18–95 years, 5.3 months' follow‐up): VE 82% (95% CI 79.5 to 84.2), n = 28,451 Confirmed symptomatic COVID‐19 b 4939 per 100,000 336 per 100,000(255 to 442) VE 93.20 (91.06 to 94.83) 31,632(2 RCTs)c ⨁⨁⨁⨁Highd — Severe or critical COVID‐19f 748 per 100,000 13 per 100,000(3 to 54) VE 98.20 (92.80 to 99.60) 28,451(1 RCT)g ⨁⨁⨁⨁Highd — All‐cause mortalityf 106 per 100,000 112 per 100,000(57 to 222) RR 1.06(0.54 to 2.10) 30,346(1 RCT)g ⨁⨁◯◯Lowh 1 additional trial: (Ali 2021 (adolescents aged 12–17 years)) reported on this outcome in 3726 participants (2486 mRNA‐1273 and 1240 placebo). There were no events in either group and the trial did not contribute to the pooled effect estimate Systemic reactogenicity eventsi 432 per 1000 553 per 1000(527 to 579) RR 1.28(1.22 to 1.34) 34,037(2 RCTs)c ⨁⨁⨁⨁Highj — Any adverse eventk Outcome not pooled due to considerable heterogeneity (I² = 100%) between included studies: Ali 2021 (all solicited adverse events, adolescents aged 12–17 years, median 2.8 months' follow‐up): RR 1.47 (95% CI 1.41 to 1.54), n = 3726; El Sahly 2021 (all solicited adverse events, adults aged 18–95 years, 5.3 months' follow‐up): RR 2.15 (95% CI 2.11 to 2.19), n = 29,269 — 32,995(2 RCTs)c ⨁⨁◯◯Lowl — Serious adverse eventsl 1792 per 100,000 1649 per 100,000(1398 to 1936) RR 0.92(0.78 to 1.08) 34,072(2 RCTs)c ⨁⨁⨁◯Moderatem — Local reactogenicity eventsi 211 per 1000 697 per 1000(427 to 1000) RR 3.30(2.02 to 5.40) 34,037(2 RCTs)c ⨁⨁⨁⨁Highn — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).COVID‐19: coronavirus disease 2019;CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. a. Last updated: 01 March 2023 b. Follow‐up: from 14 days after dose 2 to 2.3 months (median) and 5.3 months c. Moderna TX: Ali 2021 (adolescents aged 12–17 years); El Sahly 2021 (adults aged 18–95 years) d. Despite some concerns with deviations from intervention, not downgraded for risk of bias e. Inconsistency: downgraded one level: I² = 66.37% f. Follow‐up: 5.3 months g. Moderna TX: El Sahly 2021 (adults aged 18–95 years) h. Imprecision downgraded two levels due to small number of events observed and wide CIs that encompass a potential benefit and a potential harm with the intervention i. Follow‐up: seven days j. Despite inconsistency (I² = 61%) not downgraded for inconsistency, as the same direction of effect in both effect estimates k. Follow‐up: 2.8 months (median) and 5.3 months l. Inconsistency: downgraded two levels (I² = 100%) m. Imprecision: downgraded one level due to wide CIs that encompass a potential benefit and a potential harm with the intervention. n. Despite inconsistency (I² = 99%), not downgraded for inconsistency, as the same direction of effect in both effect estimates Open in table viewerSummary of findings 3. CVnCoV – CureVac AG compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence (GRADE) Comments Risk with placebo Risk with CVnCOV Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19b 1187 per 100,000 615 per 100,000(464 to 811) VE 48.20 (31.70 to 60.90) 25,062(1 RCT)c ⊕⊕⊕⊖Moderated,e — Severe or critical COVID‐19f 82 per 100,000 30 per 100,000(7 to 82) VE 63.80 (0.00 to 91.70) 25,062(1 RCT)c ⊕⊖⊖⊖Very lowd,e,g — All‐cause mortalityh 30 per 100,000 40 per 100,000(14 to 116) RR 1.33(0.46 to 3.83) 39,529(1 RCT)c ⊕⊖⊖⊖Very lowe,g — Systemic reactogenicity eventsi 635 per 1000 940 per 1000(908 to 971) RR 1.48(1.43 to 1.53) 3982(1 RCT)c ⊕⊕⊕⊕High — Any adverse eventj 679 per 1000 965 per 1000(937 to 999) RR 1.42(1.38 to 1.47) 3982(1 RCT)c ⊕⊕⊕⊖Moderatee — Serious adverse eventsk 334 per 100,000 414 per 100,000(301 to 572) RR 1.24(0.90 to 1.71) 39,529(1 RCT)c ⊕⊕⊖⊖Lowe,l — Local reactogenicity eventsi 241 per 1000 847 per 1000(782 to 920) RR 3.51(3.24 to 3.81) 3982(1 RCT)c ⊕⊕⊕⊕High — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 10 May 2022bFollow‐up: from 14 days following the second dose to 6.23 monthscCureVac AG: Kremsner 2021 (adults aged 18–98 years)dDespite some concerns with deviations from intervention, not downgraded for risk of bias.eIndirectness: downgraded one level as data are from interim analyses of the trial and from the available information it is unclear whether these were preplanned.fFollow‐up: from seven days following the second dose to six monthsgImprecision: downgraded two levels due to small number of events observed and wide CIs that encompass a potential benefit and a potential harm with the intervention.hFollow‐up: 6.23 monthsiFollow‐up: seven daysjFollow‐up: one monthkFollow‐up: 1.7 monthslImprecision: downgraded one level due to wide CIs consistent with the possibility of benefit and the possibility of harm. Open in table viewerSummary of findings 4. ChAdOx1 – AstraZeneca + University of Oxford compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence Comments Risk with placebo Risk with ChAdOx1 Confirmed SARS‐CoV‐2 infectionb 3199 per 100,000 1300 per 100,000(1017 to 1663) VE 59.35 (48.00 to 68.22) 43,390(5 RCTs)c ⊕⊕⊕⊖Moderated,e Substantial heterogeneity (I² = 68%) between included studies: Falsey 2021 (VE 64.35%, 95% CI 56.10% to 71.00%; n = 26,212); Voysey 2021a (VE 54.10%, 95% CI 44.70% to 61.90%; n = 17,178) Confirmed symptomatic COVID‐19b 2207 per 100,000 657 per 100,000(516 to 836) VE 70.23 (62.10 to 76.62) 43,390(5 RCTs)c ⊕⊕⊕⊕Highd — Severe or critical COVID‐19 Outcome not yet measured or reported All‐cause mortalityf 52 per 100,000 25 per 100,000(10 to 59) RR 0.48(0.20 to 1.14) 56,727(5 RCTs)g ⊕⊕⊖⊖Lowh 2 additional trials (Asano 2022; Kulkarni 2021) reported this outcome in 1392 participants (192 ChAdOx1 versus 64 placebo and 900 SII‐ChAdOx1 versus 300 placebo, respectively). There were no events in either group in either trial and they did not contribute to the pooled effect estimate. Systemic reactogenicity eventsi 141 per 1000 553 per 1000(297 to 1000) RR 3.93(2.11 to 7.29) 256(1 RCT)j ⊕⊕⊕⊖Moderatek — Any adverse eventl Outcome not pooled due to considerable heterogeneity (I² = 90%) between included studies: Asano 2022 (RR 2.54, 95% CI 1.73 to 3.74; n = 256); Falsey 2021 (RR 1.37, 95% CI 1.33 to 1.42; n = 32,379); Kulkarni 2021 (RR 1.39, 95% CI 1.12 to 1.74; n = 1200); Voysey 2021a (RR 0.74, 95% CI 0.56 to 0.96; n = 23,745) — 57,580(7 RCTs)m ⊕⊕⊖⊖Lown — Serious adverse eventso 794 per 100,000 699 per 100,000(572 to 850) RR 0.88(0.72 to 1.07) 58,182(7 RCTs)p ⊕⊕⊕⊖Moderateq — Local reactogenicity eventsi 94 per 1000 604 per 1000(279 to 1000) RR 6.44(2.98 to 13.92) 256(1 RCT)j ⊕⊕⊕⊖Moderatek,r — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 4 May 2022bFollow‐up: from 14 days after second dose up to 1.34 months (median) and 2 months (median)cFalsey 2021; Voysey 2021a (data from four pooled RCTs)dDespite some concerns with deviations from intervention, not downgraded for risk of bias.eInconsistency: downgraded one level (I² = 68%).fFollow‐up: 2 months, 4.2 months and 2 months (median)gFalsey 2021; Voysey 2021a (data from four pooled RCTs); Madhi 2021a (participants with HIV, trial already counted in Voysey 2021a)hImprecision: downgraded two levels due to small number of events observed and wide CIs that encompass a potential benefit and a potential harm with the intervention.iFollow‐up: seven daysjAsano 2022kImprecision: downgraded one level due to low number of participants/few events observed.lFollow‐up: 1 month, 1.16 months, 1.9 months, and 3.4 monthsmAsano 2022; Falsey 2021; Kulkarni 2021; Voysey 2021a (data from four pooled RCTs)nInconsistency: downgraded two levels (I² = 90%).oFollow‐up: 1 month, 1.9 months, 6 months, and 3.64 months (median)pAsano 2022; Falsey 2021; Kulkarni 2021; Voysey 2021a (data from four pooled RCTs). Madhi 2021a (participants with HIV, trial already counted in Voysey 2021a)qImprecision: downgraded one level due to wide CIs consistent with the possibility of benefit and the possibility of no effect.rDespite some concerns with selection of reported results, not downgraded for risk of bias. Open in table viewerSummary of findings 5. SII‐ChAdOx1 – Serum Institute of India/AstraZeneca + University of Oxford compared to ChAdOx1 – University of Oxford for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with ChAdOx1 Risk with SII‐ChAdOx1 Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19 Outcome not yet measured or reported Severe or critical COVID‐19 Outcome not yet measured or reported All‐cause mortality — — — — — 1 study reported this outcome in 400 participants (Kulkarni 2021). There were no events in either group and no effect estimate could be calculated. Systemic reactogenicity eventsb 390 per 1000 285 per 1000(211 to 382) RR 0.73(0.54 to 0.98) 400(1 RCT)c ⊕⊕⊕⊖Moderated — Any adverse evente 200 per 1000 166 per 1000(104 to 266) RR 0.83(0.52 to 1.33) 400(1 RCT)c ⊕⊕⊖⊖Lowf — Serious adverse eventsg 2000 per 100,000 1000 per 100,000(160 to 5900) RR 0.50(0.08 to 2.95) 400(1 RCT)c ⊕⊕⊖⊖Lowf — Local reactogenicity eventsb 360 per 1000 274 per 1000(198 to 378) RR 0.76(0.55 to 1.05) 400(1 RCT)c ⊕⊕⊖⊖Lowh — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 10 May 2022bFollow‐up: seven dayscKulkarni 2021dImprecision: downgraded one level due to low number of events/participants.eFollow‐up: 1.9 monthsfImprecision: downgraded two levels due to wide CIs consistent with the possibility of benefit and the possibility of harm and low number of events/participants.gFollow‐up: six monthshImprecision: downgraded two levels due to wide CIs consistent with the possibility of no effect and the possibility of benefit and low number of events/participants. Open in table viewerSummary of findings 6. AD26.COV2.S – Janssen Pharmaceutical Companies compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with placebo Risk with AD26.COV2.S Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19b 1796 per 100,000 594 per 100,000(478 to 735) VE 66.90 (59.10 to 73.40) 39,058(1 RCT)c ⊕⊕⊕⊕Highd — Severe or critical COVID‐19b 409 per 100,000 97 per 100,000(51 to 172) VE 76.30 (57.90 to 87.50) 39,058(1 RCT)c ⊕⊕⊕⊕Highd — All‐cause mortalityb 91 per 100,000 23 per 100,000(8 to 61) RR 0.25(0.09 to 0.67) 43,783(1 RCT)c ⊕⊕⊕⊕High — Serious adverse eventsb 448 per 100,000 412 per 100,000(309 to 546) RR 0.92(0.69 to 1.22) 43,783(1 RCT)c ⊕⊕⊕⊖Moderatej — Systemic reactogenicity eventse 34,575 per 100,000 63,273 per 100,000(44,602 to 89,896) RR 1.83(1.29 to 2.60) 7222(2 RCTs)f ⊕⊕⊕⊕Highd,g — Any adverse eventh Outcome not pooled due to considerable heterogeneity (I² = 96%) between included studies: Sadoff 2021a (RR 1.09, 95% CI 0.96 to 1.24; n = 6736); Sadoff 2021b (RR 2.31, 95% CI 1.80 to 2.97; n = 486) — 7222(2 RCTs)f ⊕⊕⊖⊖Lowd,i — *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 4 May 2022bFollow‐up: 1.9 months (median)cSadoff 2021bdDespite some concerns with deviations from intervention, not downgraded for risk of bias.eFollow‐up: seven days and 14 daysfSadoff 2021a; Sadoff 2021bgDespite I² = 83%, not downgraded for inconsistency, as the same direction of effect in both effect estimates.hFollow‐up: 0.23 months and 0.92 monthsiInconsistency: downgraded two levels (I² = 96%).jImprecision: downgraded one level due to wide CIs consistent with the possibility of no effect and the possibility of benefit.kFollow‐up: seven dayslDespite I² = 84%, not downgraded for inconsistency, as the same direction of effect in both effect estimates. Open in table viewerSummary of findings 7. Gam‐COVID‐VAC – Sputnik V compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with placebo Risk with Gam‐COVID‐VAC Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19b 1022 per 100,000 92 per 100,000(51 to 167) VE 91.10 (83.80 to 95.10) 18,695(1 RCT)c ⊕⊕⊕⊖Moderated,e — Severe or critical COVID‐19b 408 per 100,000 0 per 100,000(0 to 23) VE 100.00 (94.40 to 100.00) 19,866(1 RCT)c ⊕⊕⊕⊖Moderated,e — All‐cause mortalityf 18 per 100,000 18 per 100,000(2 to 176) RR 0.99(0.10 to 9.54) 21,862(1 RCT)c ⊕⊖⊖⊖Very lowd,e,g — Systemic reactogenicity events Outcome not yet measured or reported Any adverse event Outcome not yet measured or reported Serious adverse eventsf 423 per 100,000 275 per 100,000(165 to 453) RR 0.65(0.39 to 1.07) 21,862(1 RCT)c ⊕⊕⊖⊖Lowd,e,h — Local reactogenicity events Outcome not yet measured or reported *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019;CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 27 May 2022bFollow‐up: from seven days after second dosecLogunov 2021dIndirectness: downgraded one level as data are from interim analyses of the trial and from the available information it is unclear whether these were preplanned.eConcern regarding the internal validity of the trial.fFollow‐up: 1.6 months (median)gImprecision: downgraded two levels due to wide CIs consistent with the possibility of benefit and the possibility of harm and few events.hImprecision: downgraded one level due to wide CIs consistent with the possibility of no effect and the possibility of benefit. Open in table viewerSummary of findings 8. CoronaVac – Sinovac compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with placebo Risk with CoronaVac Confirmed SARS‐CoV‐2 infection Outcome not yet measured or reported Confirmed symptomatic COVID‐19b 2398 per 100,000 724 per 100,000(249 to 2104) VE 69.81 (12.27 to 89.61) 19,852(2 RCTs)c ⊕⊕⊖⊖Lowd,e,f Considerable heterogeneity (I² = 92%) between included studies: Tanriover 2021 (VE 83.50%, 95% CI 65.40% to 92.10%; n = 10,029); Palacios 2020 (VE 50.70%, 95% CI 35.90 to 62.00%; n = 9823) Severe or critical COVID‐19b 2 studies report on severe or critical disease due to COVID‐19: Tanriover 2021, with 0/6559 events in the CoronaVac group versus 1/3470 events in the placebo group and a VE of 100%, 95% CI (20.40% to 100.00%); and Palacios 2020, with 0/4953 events in the CoronaVac group and 6/4870 events in the placebo group and a VE of 100%, 95% CI (16.90% to 100.00%). (Note: estimates could not be pooled due to asymmetry in the CIs) — 19,852(2 RCTs)c ⊕⊕⊖⊖Lowd,g — All‐cause mortalityh 20 per 100,000 10 per 100,000(1 to 113) RR 0.50(0.05 to 5.52) 22,610(2 RCTs)c ⊕⊕⊖⊖Lowi — Systemic reactogenicity eventsj 409 per 1000 487 per 1000(409 to 581) RR 1.19(1.00 to 1.42) 23,966(6 RCTs)k ⊕⊕⊖⊖Lowl,m,n — Any adverse evento 531 per 1000 579 per 1000(568 to 590) RR 1.09(1.07 to 1.11) 23,367(6 RCTs)p ⊕⊕⊕⊕Highq — Serious adverse eventsr 372 per 100,000 361 per 100,000(231 to 562) RR 0.97(0.62 to 1.51) 23,139(4 RCTs)s ⊕⊕⊖⊖Lowi,q 2 additional trials (Bueno 2021; Zhang 2021) reported this outcome in 482 participants (270 versus 164 and 24 versus 24 respectively, receiving CoronaVac versus placebo). There were no events in either group and the trials did not contribute to the pooled effect estimate. Local reactogenicity eventsj 227 per 1000 400 per 1000(384 to 414) RR 1.76(1.69 to 1.82) 23,962(6 RCTs)k ⊕⊕⊕⊕Highl — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 4 May 2022bFollow‐up: from 14 days after the second dose up to two months (median)cPalacios 2020; Tanriover 2021dDespite some concerns with deviations from intervention, not downgraded for risk of bias.eInconsistency: downgraded one level (I² = 92%).fImprecision: downgraded one level due to wide CIs consistent with the possibility of benefit and the possibility of harm.gImprecision: downgraded two levels due to low number of events and wide CIs.hFollow‐up: 1.4 and 2 months (median)iImprecision: downgraded two levels due to wide CIs consistent with the possibility of benefit and the possibility of harm and few events.jFollow‐up: 7–28 dayskBueno 2021; Fadlyana 2021; Palacios 2020; Tanriover 2021; Wu 2021a; Zhang 2021lDespite some concerns with adequate randomisation, deviation from intended intervention, missing data, and selection of reported results not downgraded for risk of bias.mInconsistency: downgraded one level (I² = 55%).nImprecision: downgraded one level due to wide CIs consistent with the possibility of no effect and the possibility of harm.oFollow‐up: one to three months (median)pBueno 2021; Han 2021; Palacios 2020; Tanriover 2021; Wu 2021a; Zhang 2021qDespite some concerns with adequate randomisation, not downgraded for risk of bias.rFollow‐up: 4.1 months, 2 months (median), 3 months (median)sHan 2021; Palacios 2020; Tanriover 2021; Wu 2021a Open in table viewerSummary of findings 9. WIBP‐CorV – Sinopharm‐Wuhan compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants Certainty of the evidence(GRADE) Comments Risk with placebo Risk with WIBP‐CorV Confirmed SARS‐CoV‐2 infectionb 912 per 100,000 328 per 100,000(231 to 467) VE 64.00 (48.80 to 74.70) 25,449(1 RCT)c ⊕⊕⊕⊕Highd — Confirmed symptomatic COVID‐19b 746 per 100,000 203 per 100,000(131 to 313) VE 72.80 (58.10 to 82.40) 25,480(1 RCT)c ⊕⊕⊕⊕Highd — Severe or critical COVID‐19 Outcome not yet measured or reported All‐cause mortality — — — — — 1 trial reported on this outcome in 26,917 participants (13,464 WIBP‐CorV versus 13,453 placebo) (Al Kaabi 2021). There were no events in either group and no effect estimate could be calculated for this outcome. Systemic reactogenicity eventse 278 per 1000 275 per 1000(264 to 286) RR 0.99(0.95 to 1.03) 27,029(2 RCTs)f ⊕⊕⊕⊕Highg — Any adverse eventh 504 per 1000 484 per 1000(469 to 494) RR 0.96(0.93 to 0.98) 27,029(2 RCTs)f ⊕⊕⊕⊕High — Serious adverse eventsi 579 per 100,000 480 per 100,000(347 to 665) RR 0.83(0.60 to 1.15) 27,029(2 RCTs)f ⊕⊕⊖⊖Lowg,j — Local reactogenicity eventsk 290 per 1000 255 per 1000(247 to 267) RR 0.88(0.85 to 0.92) 27,029(2 RCTs)f ⊕⊕⊕⊕Highg — *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. aLast updated: 4 May 2022bFollow‐up: from 2 weeks after the second dose up to 2.6 months (median)cAl Kaabi 2021dDespite some concerns with deviations from intervention, not downgraded for risk of bias.eFollow‐up: seven days and 28 daysfAl Kaabi 2021; Guo 2021gDespite some concerns with adequate randomisation, not downgraded for risk of bias.hFollow‐up: one monthiFollow‐up: 1.6 and 2.6 months (median)jImprecision: downgraded two levels due to wide CIs consistent with the possibility of no effect and the possibility of benefit and few events.kFollow‐up: seven days Open in table viewerSummary of findings 10. BBIBP‐CorV – Sinopharm‐Beijing compared to placebo for vaccination against COVID‐19a Outcomes Anticipated absolute effects* (95% CI) Relative effect(95% CI) № of participants(studies) Certainty of the evidence(GRADE) Comments Risk with placebo Risk with BBIBP‐CorV Confirmed SARS‐CoV‐2 infectionb 912 per 100,000 242 per 100,000(162 to 359) VE 73.50 (60.60 to 82.20) 25,435(1 RCT)c ⊕⊕⊕⊕Highd — Confirmed symptomatic COVID‐19b 746 per 100,000 163 per 100,000(102 to 263) VE 78.10 (64.80 to 86.30) 25,463(1 RCT)c ⊕⊕⊕⊕Highd — Severe or critical COVID‐19 Outcome not yet measured or reported All‐cause mortality — — — — — 1 study reported this outcome in 26,924 participants (13,471 BBIBP‐CorV versus 13,453 placebo) (Al Kaabi 2021). There were no events in either group and no effect estimate could be calculated for this outcome. Systemic reactogenicity eventse 274 per 1000 288 per 1000(236 to 351) RR 1.05(0.86 to 1.28) 27,540(3 RCTs)f ⊕⊕⊕⊖Moderateg — Any adverse eventh 3 studies (n = 27,540) reported any adverse event with 1 month or 2.9 months' follow‐up. 2 of the studies reported an effect estimate in favour of BBIBP‐CorV: 1 with RR 0.91, 95% CI 0.89 to 0.94; n = 26,924; and 1 with CIs crossing the line of no effect (RR 0.83, 95% CI 0.36 to 1.95; n = 112). 1 study reported an effect estimate in favour of placebo with CIs not crossing the line of null effect (RR 2.05, 95% CI 1.47 to 2.87; n = 504) — 26,924(3 RCTs)f ⊕⊕⊖⊖Lowi,j — Serious adverse eventsk 580 per 100,000 441 per 100,000(313 to 615) RR 0.76(0.54 to 1.06) 26,924(1 RCT)c ⊕⊕⊖⊖Lowl 1 additional study reported this outcome in 112 participants (84 BBIBP‐CorV versus 28 placebo) (Xia 2020). There were no events in either group and the trial did not contribute to the effect estimate. Local reactogenicity eventse 3 studies (n = 27,540) reported local adverse events with 7 days' follow‐up. 1 study reported an effect estimate in favour of BBIBP‐CorV: RR 0.71, 95% CI 0.68 to 0.74; n = 26,924. 2 studies reported an effect estimate in favour of placebo with CIs not crossing the line of null effect (RR 10.00, 95% CI 2.36 to 42.34; n = 504 and RR 3.33, 95% CI 0.45 to 24.89; n = 112). — 26,924(3 RCTs)f ⊕⊕⊖⊖Lowi,j — *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). COVID‐19: coronavirus disease 2019CI: confidence interval; RCT: randomized controlled trial; RR: risk ratio; SARS‐CoV‐2: severe acute respiratory syndrome coronavirus 2; VE: vaccine efficacy. GRADE Working Group grades of evidenceHigh certainty: we are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.Very low certainty: we ha
|
|
Scooped by
Gilbert C FAURE
July 22, 2023 5:20 AM
|
The proliferation of fake news on social media has become a major societal concern which has been shown to impact elections, referenda, and effective public health messaging (Lewandowsky et al., 2017).
|
|
Scooped by
Gilbert C FAURE
March 9, 2023 10:15 AM
|
Concerns regarding the safety of COVID-19 vaccination have caused hesitancy and lowered uptake globally. While vaccine hesitancy is documented globally, some continents, countries, ethnic groups an...
|
|
Scooped by
Gilbert C FAURE
January 11, 2023 1:00 PM
|
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continued to mutate and spread in 2022 despite the introduction of safe, effective vaccines and medications. Vaccine hesitancy remains substantial, fueled in part by misinformation. Our third study of Coronavirus Disease 2019 (COVID-19) vaccine hesitancy among 23,000 respondents in 23 countries (Brazil, Canada, China, Ecuador, France, Germany, Ghana, India, Italy, Kenya, Mexico, Nigeria, Peru, Poland, Russia, Singapore, South Africa, South Korea, Spain, Sweden, Turkey, the United Kingdom and the United States), surveyed from 29 June to 10 July 2022, found willingness to accept vaccination at 79.1%, up 5.2% from June 2021. Hesitancy increased in eight countries, however, ranging from 1.0% (United Kingdom) to 21.1% (South Africa). Almost one in eight (12.1%) vaccinated respondents are hesitant about booster doses. Overall support for vaccinating children under 18 years of age increased slightly but declined among parents who were personally hesitant. Almost two in five (38.6%) respondents reported paying less attention to new COVID-19 information than previously, and support for vaccination mandates decreased. Almost a quarter (24%) of those who became ill reported taking medications to combat COVID-19 symptoms. Vaccination remains a cornerstone of the COVID-19 pandemic response, but broad public support remains elusive. These data can be used by health system decisionmakers, practitioners, advocates and researchers to address COVID-19 vaccine hesitancy more effectively. In the third annual iteration of a survey assessing vaccine confidence in 23 high-income, middle-income and low-income countries, although results were heteregeous across countries, overall willingness to accept a COVID-19 vaccine was found to have increased.
|
|
Scooped by
Gilbert C FAURE
October 17, 2022 10:13 AM
|
Félicitons les chercheurs à l'origine d'initiatives, encore trop rares, pour signaler et faire rétracter des articles honteux pour la science. Je vous suggère de lire deux articles de la même équipe d'auteurs : Robert J, et coll. Covidiots et cancer. Y-a-t-il une ânerie qu'ILS n'ont pas proférée ? Innovations &…
|
|
Scooped by
Gilbert C FAURE
May 25, 2022 11:05 AM
|
Background: China is at the forefront of global efforts to develop COVID-19 vaccines and has five fast-tracked candidates at the final-stage, large-scale human clinical trials testing phase. Vaccine-promoting policymaking for public engagement is a prerequisite for social mobilization. However, making an informed and judicious choice is a dilemma for the Chinese government in the vaccine promotion context.
Objective: In this study, public opinions in China were analyzed via dialogues on Chinese social media, based on which Chinese netizens’ views on COVID-19 vaccines and vaccination were investigated. We also aimed to develop strategies for promoting vaccination programs in China based on an in-depth understanding of the challenges in risk communication and social mobilization.
Methods: We proposed a novel behavioral dynamics model, SRS/I (susceptible-reading-susceptible/immune), to analyze opinion transmission paradigms on Chinese social media. Coupled with a meta-analysis and natural language processing techniques, the emotion polarity of individual opinions was examined in their given context.
Results: We collected more than 1.75 million Weibo messages about COVID-19 vaccines from January to October 2020. According to the public opinion reproduction ratio (R0), the dynamic propagation of those messages can be classified into three periods: the ferment period (R01=1.1360), the revolution period (R02=2.8278), and the transmission period (R03=3.0729). Topics on COVID-19 vaccine acceptance in China include price and side effects. From September to October, Weibo users claimed that the vaccine was overpriced, making up 18.3% (n=899) of messages; 38.1% (n=81,909) of relevant topics on Weibo received likes. On the contrary, the number of messages that considered the vaccine to be reasonably priced was twice as high but received fewer likes, accounting for 25.0% (n=53,693). In addition, we obtained 441 (47.7%) positive and 295 (31.9%) negative Weibo messages about side effects. Interestingly, inactivated vaccines instigated more heated discussions than any other vaccine type. The discussions, forwards, comments, and likes associated with topics related to inactivated vaccines accounted for 53% (n=588), 42% (n=3072), 56% (n=3671), and 49% (n=17,940), respectively, of the total activity associated with the five types of vaccines in China.
Conclusions: Most Chinese netizens believe that the vaccine is less expensive than previously thought, while some claim they cannot afford it for their entire family. The findings demonstrate that Chinese individuals are inclined to be positive about side effects over time and are proud of China’s involvement with vaccine development. Nevertheless, they have a collective misunderstanding about inactivated vaccines, insisting that inactivated vaccines are safer than other vaccines. Reflecting on netizens’ collective responses, the unfolding determinants of COVID-19 vaccine acceptance provide illuminating benchmarks for vaccine-promoting policies.
|
|
Scooped by
Gilbert C FAURE
May 13, 2022 11:25 AM
|
Yuki Senoo1, Akihiko Ozaki2, Makoto Watanabe3, Tetsuya Tanimoto11Medical Governance Research Institute, Tokyo, Japan.2Department of Breast Surgery, Jyoban Hospital of Tokiwa Foundation, Fukushima, Japan3Tansa, Tokyo, Japan.In an era where “fake news” and biased information are shared in the traditional press and on social media, collaboration between physicians and journalists is increasingly important to help disseminate accurate and trustworthy health information to the general public.1 Our experience from Japan shows how independent investigative journalists and physicians can collaborate together to publish unbiased and objective health information.In today’s competitive market in Japan, most traditional media increasingly rely on advertising revenue from for-profit organizations.23 There are concerns that this financial model has forced some media outlets to refrain from criticising advertisers, or running paid product promotions without making it clear to readers that these are advertisements.45 This has impaired their independence and undermines their credibility among the public in Japan. Because pharmaceuticals and medical device companies often sponsor the mass media, there are concerns about the impact that this has on healthcare reports and making sure that these are unbiased and free from the influence of commercial organizations.6In this context, investigative media groups that mainly obtain funds from donations or an independent membership system could play an important role in healthcare reporting and dissemination.1 A notable example is ProPublica in the United States, which often focuses on medical issues in the country.1 ProPublica created a free public database called Dollars for Doc (https://www.propublica.org/datastore/dataset/dollars-for-docs-2013-2016) similar to the Open Payments Data by the US Government (https://openpaymentsdata.cms.gov), where they publish details of payments made to physicians from pharmaceuticals and medical devices companies, using data disclosed under the US’s Sunshine Act. ProPublica have used their position to shine a light on other examples of commercial interests in healthcare as well.7This type of business model that relies on donations or membership is notoriously unstable, particularly at the early development stage, when a media group does not have sufficient social recognition and a fragile financial base. To provide professional expertise for investigations related to health, our team of physicians partnered with the Japanese investigative journalist group Tansa (originally called Waseda Chronicle).8 In 2017, Tansa was established by journalists to promote journalistic independence. It launched a crowdfunding platform,9 and their initial project uncovered that some pharmaceutical companies paid for seemingly neutral health reports about their products published in newspaper articles as a stealth marketing strategy.10Tansa has focused on health issues since its foundation, paying particular attention to financial conflicts of interest (FCOIs) between pharmaceutical companies and the healthcare sector.4 Japan has no laws similar to the Sunshine Act in the US, and lags behind in establishing a public database similar to the Open Payments Database.11 This is because it has been difficult to reach an agreement between physicians, pharma companies, the medical devices industry, and the government on improving the transparency of FCOIs.To help overcome this, in January 2019, we launched our first freely accessible database. It is similar to Dollars for Doc by ProPublica and was created through collaboration between physicians and journalists. Doctors contributed to the project by working with the journalists on interpreting the data and providing insights from clinical practice. The database discloses payments made by pharmaceutical companies to healthcare professionals in the fiscal year of 2016 to 2018.1112 In Japan, payments data have been separately disclosed by major pharmaceutical companies in a non-user-friendly format, and previously it was impossible to analyse the whole picture.11 Although the information is limited to data on honorariums to healthcare professionals provided by Japanese pharmaceutical companies, through our database, anyone can freely access details of pharmaceutical payments made to physicians for the first time in Japan.12 The next step has been to publish pharmaceutical payments made to healthcare organizations.111314151617The challenge of this work lies in its long term continuity since our activities are not supported by a stable funding source. Arguably, our database should be a public infrastructure run by the government or related public organizations, but that is unlikely to materialize in the foreseeable future in Japan. Our experience highlights the way in which financial independence, a lack of association with any potential conflicting actors or agencies, and equitable collaboration between physicians and journalists are key components in ensuring the dissemination of correct, reliable, and unbiased health information.FootnotesCompeting interests: Dr Ozaki reports personal fees from Medical Network Systems (MNES) Inc., outside the submitted work. Dr Tanimoto reports personal fees from Medical Network Systems (MNES) Inc., and Bionics co., Lt outside the submitted work. All other authors declare that they have no competing interests.Acknowledgments:The authors thank Andy Crump for his constructive opinions and professional English editing.FundingThe Medical Governance Research Institution is a non-profit organisation that has received donations from various individuals, industries, and organizations, including donations from the pharmaceutical industry, notably from Ain Pharmacies. Ain Pharmacies were not involved in the design of this opinion piece, the work carried out, the interpretation of the study findings or decision to submit the manuscript for publication.References↵Arora VM, Rousseau D, Schwitzer G. Why Bolstering Trust in Journalism Could Help Strengthen Trust in Medicine. JAMA2019;321:2159-60. doi:10.1001/jama.2019.0636. pmid:31081867OpenUrlCrossRefPubMed↵Brasor P. Reporter’s death puts spotlight on shifting media landscape. The Japan Times. 2021 November 27. Available from: https://www.japantimes.co.jp/news/2021/11/27/national/media-national/japan-shifting-media-landscape/ [Accessed 2022 April 13].↵Takada Y, Harada Y. The Media Content Market in Japan and Its Recent Changes. Keio Commun Rev2011;33:5-24.OpenUrl↵Watanabe M. Big pharma paid doctors 26.6 billion yen in a single year. Tansa. 2018 October 27. Available from: https://en.tansajp.org/investigativejournal/567/ [Accessed 2022 April 13].↵Roy A, Chattopadhyay SP. Stealth marketing as a strategy. Bus Horiz2010;53:69-79. doi:10.1016/j.bushor.2009.09.004.OpenUrlCrossRef↵Schwitzer G. Conflicts of interest in health care journalism. Who’s watching the watchdogs? 2017 June 19. Available from: https://centerforhealthjournalism.org/2017/06/16/conflicts-interest-health-care-journalism-who's-watching-watchdogs-we-are-part-1-3 [Accessed 2022 April 13].↵ProPublica. Opioid Billionaires. Available from: https://www.propublica.org/series/opioid-billionaires [Accessed 13 April 2022].↵Tansa. 2017. Available from: https://en.wasedachronicle.org/about [Accessed 2022 April 13].↵Tansa. Donation platform for “Waseda Chronicle” to continue publishing investigative series “Advertorial- Incentive fee paid to Kyodo News by Nippon Dentsu group for successful publication” [in Japanese]. 2017. Available from: https://motion-gallery.net/projects/waseda-journalism [Accessed 2022 April 13].↵Tansa. Journalism for Sale. 2020. Available from: https://en.tansajp.org/investigativejournal_category/buying-articles/ [Accessed 2022 April 13].↵Ozaki A, Saito H, Senoo Y, et al. Overview and transparency of non-research payments to healthcare organizations and healthcare professionals from pharmaceutical companies in Japan: Analysis of payment data in 2016. Health Policy2020;124:727-35. doi:10.1016/j.healthpol.2020.03.011. pmid:32439213OpenUrlCrossRefPubMed↵Tansa. Money Database “Pharmaceutical companies and medical doctors”. Available from: https://db.tansajp.org/en [Accessed 2022 April 13].↵Kobashi Y, Watanabe M, Kimura H, Higuchi A, Ozaki A. Are Pharmaceutical Company Payments Incentivising Malpractice in Japanese Physicians?Int J Health Policy Manag2019;8:627-8. doi:10.15171/ijhpm.2019.60. pmid:31657193OpenUrlCrossRefPubMed↵Saito H, Ozaki A, Sawano T, Shimada Y, Tanimoto T. Evaluation of Pharmaceutical Company Payments and Conflict of Interest Disclosures Among Oncology Clinical Practice Guideline Authors in Japan. JAMA Netw Open2019;2:e192834-34. doi:10.1001/jamanetworkopen.2019.2834. pmid:31026027OpenUrlCrossRefPubMed↵Saito H, Tani Y, Ozaki A, et al. Financial ties between authors of the clinical practice guidelines and pharmaceutical companies: an example from Japan. Clin Microbiol Infect2019;25:1304-6. doi:10.1016/j.cmi.2019.07.025. pmid:31401175OpenUrlCrossRefPubMed↵Sawano T, Ozaki A, Saito H, Shimada Y, Tanimoto T. Payments From Pharmaceutical Companies to Authors Involved in the Valsartan Scandal in Japan. JAMA Netw Open2019;2:e193817-17. doi:10.1001/jamanetworkopen.2019.3817. pmid:31099864OpenUrlCrossRefPubMed↵Saito H, Ozaki A, Kobayashi Y, Sawano T, Tanimoto T. Pharmaceutical Company Payments to Executive Board Members of Professional Medical Associations in Japan. JAMA Intern Med2019;179:578-80. doi:10.1001/jamainternmed.2018.7283. pmid:30715087OpenUrlCrossRefPubMed

|
Suggested by
LIGHTING
April 20, 2022 1:55 PM
|
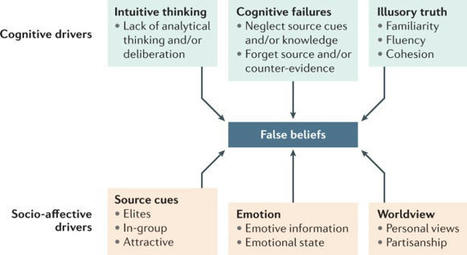
The psychological drivers of misinformation belief and its resistance to correction - Nature Review
|
|
Scooped by
Gilbert C FAURE
April 19, 2022 3:11 AM
|
Un article paru dans le magazine The Conversation et immédiatement repris par Scientific American le 22 janvier 2020 rapportait : « Les serpents – le krait chinois et le cobra chinois – pourraient être la source d'origine du coronavirus récemment découvert qui a déclenché une épidémie d'une...
|
|
Rescooped by
Gilbert C FAURE
from Veille Coronavirus - Covid-19
November 16, 2021 3:12 AM
|
Since the first case of COVID-19 was identified in the USA in January, 2020, over
46 million people in the country have tested positive for SARS-CoV-2 infection. Several
COVID-19 vaccines have received emergency use authorisations from the US Food and
Drug Administration, with the Pfizer–BioNTech vaccine receiving full approval on Aug
23, 2021. When paired with masking, physical distancing, and ventilation, COVID-19
vaccines are the best intervention to sustainably control the pandemic. However, surveys
have consistently found that a sizeable minority of US residents do not plan to get
a COVID-19 vaccine.
Via HAS-veille
|
|
Scooped by
Gilbert C FAURE
July 26, 2021 6:33 AM
|
The development of COVID-19 vaccines is occurring at unprecedented speeds, but require high coverage rates to be successful. This research examines in…
|
|
|
Scooped by
Gilbert C FAURE
December 14, 2023 11:02 AM
|
WHAT IS ALREADY KNOWN ON THIS TOPICAvailable literature has demonstrated an association between the level of public trust in scientists and adherence to protective behaviours during epidemics and has emphasised the importance of effective public health communication to ensure compliance with public health guidance.WHAT THIS STUDY ADDSThe present study found that the distrusting public sought to ‘outscience’ the scientists, questioned who was a ‘scientist’, and contended that political and economic interests controlled scientific inquiry. Definitions of ‘scientists’ and ‘scientific investigation’ and perceived roles of scientists in epidemic emergence and policymaking are more varied than prior research presumed. Our study thus extends knowledge about trust in scientists by questioning assumptions about public definitions of ‘scientist’ and ‘scientific investigation’.HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYThis study expands the scope of research on trust in scientists by investigating qualitatively public understanding and definitions of scientists, scientific investigation and uncertainty. These insights should be integrated into strengthening scientific literacy in Europe.IntroductionPreoccupations with public trust in scientists and science are not new.1 Longitudinal and multicountry surveys have assessed public confidence in science and scientists, in relation to sociodemographic factors such as age, gender, education level and political affiliation.2 3 Other studies have investigated specific factors affecting public trust in science and scientists, including perceived transparency, belief in pseudoscience,4 trust in government and corporations,5 conflicts of interest6 and historical cases of misuse of biomedical research.7 The COVID-19 pandemic accentuated public health specialists’ concerns about public trust in science and scientists,8 9 particularly because this trust is so closely linked to adherence to preventive measures, both non-pharmaceutical and vaccination.10 11 Past and current assessments of public trust in scientists and science have delineated similar profiles of social groups more or less likely to trust.10–12 Since 2020, they have also identified the global proliferation of controversies around pandemic origins, non-pharmaceutical interventions, vaccines and treatments.13 Facilitated by social media platforms and widespread anxiety in the recent pandemic crisis, certain social groups have been characterised as governed by emotion,14 irrationality,15 overconfidence16 and ignorance.17 Underpinning these studies addressing trust in scientists and science is an assumption that ‘scientists’ constitute a cohesive, homogeneous community engaged in a consensus-driven pursuit of knowledge.Dissent, however, is at the core of scientific endeavour,18 and it is crucial for producing consensus, which is often fleeting.19 The profound uncertainties and debates characterising the scientific understanding of SARS-CoV-2, COVID-19, and prevention and treatment measures mirror the dissent that Thomas Kuhn found so fundamental to the production of scientific knowledge. In his seminal work ‘The Structure of Scientific Revolutions’, Kuhn argued that scientific progress is not always linear or cumulative. Instead, it often entails ‘paradigm shifts’, in which persistent anomalies and dissenting views challenge established frameworks of understanding, catalysing their replacement by new frameworks. The profound uncertainties and debates surrounding SARS-CoV-2, COVID-19, and its prevention and treatment measures provoked such Kuhnian debates and changing frameworks. Uncertainty during the pandemic also generated public health measures based on what Eysenbach20 has described as the ‘best available evidence’, and not ‘evidence-based facts’. Two salient questions remain unexplored in the literature on trust in science and scientists. First, proliferating surveys about public ‘trust in scientists’ and ‘trust in science’ without deeper exploration of lay understanding of who qualifies as a scientist and what scientists do misrepresent the complex and contentious processes of scientific knowledge production, particularly in uncertain and volatile epidemic contexts. We need better insight into the public’s understanding of what constitutes science, who can be considered a scientist and scientists’ roles—or lack thereof—in epidemic policymaking and response. Second, although numerous studies have examined levels of confidence towards science or scientists among different social and demographic groups, as well as associations between this trust and specific non-sociodemographic factors, there is scarce exploration and analysis of why the diverse public trust or distrust science and scientists.We therefore conducted a cross-sectional mixed-methods survey among 7000 respondents in seven European countries (Belgium, France, Germany, Italy, Spain, Sweden and Ukraine) to investigate public trust in scientists engaged in COVID-19 research. Conducted in December 2020, the survey occurred at a crucial historical moment for public trust in scientists, when news of an effective COVID-19 vaccine had just been announced and plans for vaccine rollout were under way. The survey sought to identify diverse factors linked to the public trust in scientists involved in COVID-19 research, but also queried participants through closed-ended questions and text boxes about their understanding of pandemic origins and intentions to accept vaccination or specific treatments for COVID-19. Open-text responses revealed much about the public understanding of who are scientists, the work they do, the claims and practices they consider to be scientific, and the roles they and other actors have in producing knowledge to inform pandemic response.MethodsTo develop the cross-sectional mixed-methods survey, we carried out social listening (online collection and analysis) of COVID-19-related tweets in English posted by users in the European Union in May–June 2020. We employed thematic coding to identify ongoing scientific controversies, top narratives circulating about scientists, trials, vaccines and treatments, including conspiracy-related discourses. We then used the results to create a survey investigating trust in scientists and in national and international authorities and institutions and included questions about the understanding of pandemic origins, and anticipated protective practices and devices, and treatment.The cross-sectional survey, conducted by the market research firm Ipsos, was implemented through an online survey on 4–16 December 2020 among 7000 respondents in Belgium, France, Germany, Italy, Spain, Sweden and Ukraine. Following its standard protocol, Ipsos set quotas aligned with nationally representative proportions based on age (18–65 years), gender, geographical region and working status for each country. Ipsos developed a sample of participants from its existing online research panels, contacting potential participants by email to participate. When each quota was filled, Ipsos closed the quota immediately. One thousand respondents between 18 and 65 years old in each country participated. Ipsos did not survey those over age 65 years because its panel surveys cannot ensure representative sampling of this population. The following quantitative data were collected among respondents: socioeconomic and demographic characteristics, including gender identification (male/female/other/prefer not to answer); trust in sources of medical and scientific information; trust in national, European, and international institutions and authorities, as well as in pharmaceutical companies; perception of vaccine contents, purposes and safety; and political affiliation. The questionnaire included questions about participant understanding of clinical trials, perceptions of COVID-19 origins, prevention, testing, treatment preferences and anticipated COVID-19 vaccine acceptance. Trust in scientists was defined based on participants’ responses to three questions in the survey. Participants were asked to rank their level of agreement to the following statements:‘Scientists working in my country are competent to do research on COVID-19.’‘Scientists working in my country who are doing research on COVID-19 would be honest about what they discover.’‘Scientists working in my country who are doing research on COVID-19 are doing their work in the best interests of the public.’Data analysisData analyses were quantitative and qualitative. We initially conducted descriptive statistical analyses, presenting categorical variables as N (number of participants) and % (percentage from the total study population) for each category of variable. For analysis of trust, we combined the three questions above on trust into a single binary variable (trust/no trust), which served as a proxy to reflect trust in scientists. Relationships between trust in scientists and other factors (sociodemographic, information sources, personal COVID-19 experiences and beliefs in specific rumours) were analysed using an Akaike Information Criterion-based stepwise backwards multivariate regression model. We used France as the reference class. All results are expressed as ORs and 95% CIs. All quantitative analyses were performed using R software V.4.1.1.Survey participants’ open-text responses about COVID-19 treatment, vaccination and SARS-CoV-2 origins were evaluated using thematic analysis.21 We developed a global codebook and conducted inductive and deductive thematic coding using NVivo software (QSR international, V.1.7.1). We also organised our analyses to categorise descriptions of existing COVID-19 scientific research according to expressed trust in scientists, participant sentiments towards key actors and explanations of responses contending that SARS-CoV-2 was deliberately released. Blank (unanswered) text boxes were not evaluated.To ensure high-quality text analysis, a native speaker of each country language (French, Italian, Spanish, Ukrainian, German, Flemish and Swedish) performed the coding. All coders conferred frequently during the coding process to address and compare transversal codes and themes.Patient and public involvementThere were no patients involved in the study. We did not explicitly involve the public in the research questions, design, recruitment or outcome measures of the study, nor were they asked to assess the burden of time required to participate in the research. Our development of the survey tool, however, did draw on specific debates about COVID-19 on Twitter.ResultsQuantitative resultsOur sample exhibited a balanced distribution of gender and age groups. In this sample, 34% participants were not employed, 43% identified as having centrist political beliefs and most possessed at least secondary education (see online supplemental file 1).Supplemental material[bmjph-2023-000280supp001.pdf]Table 1 evaluates trust in scientists and its associations with sociodemographic characteristics, use of information sources and beliefs, and experiences with COVID-19. Statistically significant associations were observed between trust in scientists and sociodemographic characteristics (country of origin, age, level of education, political affiliation). In comparison with France, respondents residing in Belgium (OR 1.25, 95% CI 1.03 to 1.52, p<0.025), Italy (OR 1.26, CI 1.04 to 1.54, p<0.020) and Sweden (OR 1.41, CI 1.16 to 1.72, p<0.001) had higher odds of trusting scientists. In contrast, respondents in Germany (OR 0.79, CI 0.65 to 0.96, p=0.018) and Ukraine (OR 0.39, CI 0.31 to 0.49, p<0.001) were less trustful of scientists. In comparison with the youngest respondents (18–24 years old), older groups, notably those 44–54 years old (OR 1.36, CI 1.12 to 1.65, p=0.002) and 55–65 years old (OR 1.71, CI 1.41 to 2.08, p<0.001), expressed significantly more trust in scientists. Participants with secondary (OR 1.33, CI 1.05 to 1.70, p=0.018) and tertiary (OR 1.57, CI 1.24 to 1.99, p<0.001) education levels also tended to trust scientists more than those with only primary education. Those declaring a preference to vote for centre (OR 1.15, CI 1.01 to 1.32, p=0.041) and left (OR 1.59, CI 1.33 to 1.89, p<0.001) political parties showed higher levels of trust than those affiliating themselves with politically right-wing parties.View inline View popup Table 1 Relations between sociodemographic characteristics, information sources and beliefs, experience with COVID-19 and trust in scientistsUse of certain information sources about COVID-19 was also significantly associated with trust in scientists. Participants obtaining their information via traditional media (newspapers, TV, radio, etc) (OR 1.48, CI 1.28 to 1.72, p<0.001), mainstream organisational/institutional websites (OR 1.39, CI 1.24 to 1.55, p<0.001), face-to-face discussions with friends and family (OR 1.15, CI 1.02 to 1.30, p=0.016) and their healthcare environment (eg, posters in hospital waiting rooms) (OR 1.23, CI 1.07 to 1.43, p=0.005) trusted in scientists more than those who did not. Respondents who reported seeking COVID-19-related information from blogs and non-mainstream websites (OR 0.81, CI 0.68 to 0.97, p=0.024), online conversations (OR 0.84, CI 0.72 to 0.97, p=0.016) and those who stated they did not use any information sources listed in the survey (OR 0.62, CI 0.40 to 0.94, p=0.027) were less trustful of scientists than those who did not.Experience with COVID-19 was also associated with trust in scientists, including having a close family member or friend with COVID-19-like symptoms (OR 1.18, CI 1.03 to 1.35, p=0.017) or knowing someone who had been in an intensive care unit (ICU) due to COVID-19 (OR 1.21, CI 1.01 to 1.44, p=0.038). In addition, not knowing someone admitted to an ICU also yielded higher odds of trusting scientists (OR 1.24, CI 1.08 to 1.42, p=0.002).Embracing narratives that significantly deviated from mainstream scientific debates about SARS-CoV-2 origins and purported roles of certain technologies in COVID-19 was significantly associated with decreased trust in scientists. Participants contending that COVID-19 was deliberately released from a laboratory (OR 0.43, CI 0.37 to 0.50, p<0.001) and that COVID-19 symptoms worsened with exposure to 5G technology (OR 0.53, CI 0,37 to 0.75, p<0.001) had much lower odds of trusting scientists than those indicating that they did not believe in these rumours.The distribution of responses to COVID-19 origins and aggravators differed across countries, as shown in figure 1. In all countries except Ukraine, respondents most frequently attributed the pandemic origin to a zoonotic spillover. In Ukraine, however, respondents most frequently selected the response that the pandemic resulted from a deliberate viral release. Across all countries, at least one-third of respondents believed that the virus was accidentally or deliberately released. Claims that COVID-19 symptoms are caused or worsened by 5G technology were rare in all countries.<img src="https://bmjpublichealth.bmj.com/content/bmjph/1/1/e000280/F1.medium.gif"; class="highwire-fragment fragment-image" width="440" alt="Figure 1" height="255">Download figure Open in new tab Download powerpoint Figure 1 COVID-19 origins and aggravators by country.Table 2 shows that participants trusting scientists were more likely to believe that the COVID-19 pandemic origins resulted from a zoonotic spillover (OR 2.82, CI 2.55, 3.12, p<0.001) and to accept a COVID-19 vaccine (OR 3.67 OR, CI 3.29, 4.09, p<0.001). The relationship between trust in scientists and acceptance of paracetamol, the sole recommended treatment at the time, was not statistically significant (OR 1.1, CI 0.89, 1.35, p=0.4).View inline View popup Table 2 Perceptions of COVID-19 origins and anticipated vaccine or paracetamol treatment acceptance among respondents trusting scientistsQualitative resultsOur qualitative results centred on text responses to queries about pandemic origins, intentions to accept specific COVID-19 treatments and anticipated COVID-19 vaccine acceptance. Overall, participants provided a total of 8404 open-text responses explaining their theories of pandemic origins (1859 responses) and intentions to accept a specific COVID-19 treatment (2205 responses) and a COVID-19 vaccine (4340 responses) (online supplemental file 2).Supplemental material[bmjph-2023-000280supp002.pdf]Roughly equal numbers of respondents trusting and not trusting scientists frequently referred to scientific research to justify their responses to questions about COVID-19 origins and intentions to accept COVID-19 vaccination and paracetamol as COVID-19 treatment (table 3). Participants also signalled a lack of data to support claims about treatments and vaccines. Those not trusting scientists tended to claim that existing knowledge was insufficient or that more research was needed. Crucially, these respondents mobilised apparently scientific justifications to support their contentions. One participant denying the pandemic’s cause was a zoonotic spillover argued, ‘No link established for animal transmission to date; ‘surprising’ viral sequence…’View inline View popup Table 3 Trust in scientists and descriptions of existing COVID-19 scientific researchRespondents not trusting scientists expressed roughly equally positive and negative comments about scientists (online supplemental file 3). Those not trusting scientists sometimes underscored scientists’ prowess to support their own convictions the virus was released intentionally. Still others lauded certain researchers who have taken stances against the dominant scientific discourse, notably Didier Raoult, who claimed that hydroxychloroquine was an effective COVID-19 treatment, and Franco Trinca, who advocated ‘free choice’ regarding COVID-19 vaccine uptake. Both Raoult (French dataset) and Trinca (Italian dataset) were applauded for their willingness to treat patients with drugs not recommended by national authorities (ie, hydroxychloroquine). Another respondent cited a ‘Nobel prize winner’ as a source for the claim that SARS-CoV-2 was not a ‘natural’ virus. Participants trusting scientists responded somewhat more positively about scientists but mentioned no individual scientists in their responses. Few scientists were named and applauded for their merits, but those mentioned had all challenged mainstream scientific discourses about COVID-19 origins and treatments.Supplemental material[bmjph-2023-000280supp003.pdf]Many respondents, although neither lauding or attacking scientists, suggested that scientists themselves were powerless, serving instead more powerful actors, including states, economic interests and pharmaceutical companies. Such reflections appeared in claims that scientists had developed COVID-19 vaccines long before the pandemic for authorities or had inserted microchips to control populations in these vaccines.Even more revealing were open-text responses concerning pandemic origins, showing scientists as neither the most cited nor the most significant actors. Among participants contending that SARS-CoV-2 was deliberately released, we identified four themes in all country respondents (table 4). First, some respondents argued that the deliberate viral release was to impose demographic control, to reduce elderly and poor populations, and thus to decrease public spending on pensions, healthcare or social welfare. A second theme contended that the pandemic bolstered a country’s geopolitical standing. A French respondent, for instance, designated China as the cause of the pandemic, waging ‘a war without arms, aimed at weakening Europe and the U.S.’. China was the focus of much criticism (see also online supplemental file 3), with respondents contending that Chinese authorities had deliberately released the virus as part of its geopolitical strategy. Third, respondents argued the deliberate viral release was designed to reap financial benefits. A Ukrainian respondent contended that the pandemic was a means ‘to cause the final collapse in third world countries and further manipulate them for their own enrichment. Western European countries, the United States and China are enriching themselves.’ An Italian participant saw the beneficiaries as more circumscribed, arguing: ‘Behind every world catastrophe there is always a small circle of people … beyond nationality, ethnicity and government office…who make a huge profit at the expense of the general community’. Participants not trusting scientists were highly critical of pharmaceutical companies, arguing that these companies had deliberately released the pandemic virus to profit from vaccines. Finally, respondents contended that governments or ‘politicians’ released the virus to increase control over citizens. Another Italian participant observed, ‘The scoop is to further the Great Reset and create an Orwellian-style dictatorial world through the excuse of the pandemic’. A handful of participants offered other explanations, which were too diffuse or unclear to categorise.View inline View popup Table 4 Frequency (Freq) of most common narratives in open-text responses about deliberate COVID-19 releaseAlthough these narratives appeared in all seven countries, their prevalence varied (see table 4). Open-text responses in Belgium, France and Ukraine highlighted demographic control as an explanation for the virus’s deliberate release, whereas Italy and Sweden tended to highlight its release as generating geopolitical advantages to other countries.DiscussionThe present study investigated factors associated with European public trust in scientists at a crucial moment in the COVID-19 pandemic, exploring text responses concerning COVID-19 origins and intentions to accept COVID-19 treatments and vaccines. Our findings indicate higher levels of trust in scientists within higher-income countries of Belgium, Italy and Sweden, and less trust in Ukraine, a lower-income country. Consistent with previous research,22 23 we observed higher trust among older individuals, those in higher-income countries and those with higher educational levels. In contrast to a Wellcome Trust study,22 we found greater trust among respondents over 45 years old.Political affiliation appears to play a role in trust levels. Our study suggests that those aligned with the political left and centre exhibited greater trust in scientists compared with their right-leaning counterparts, aligning with trends observed in the USA and Europe, where public perceptions of science have been influenced by political discourse.24 25 In contrast, one German study examining changing levels of trust in science over the pandemic reported that trust increased at its outset but declined over time, more so among right-wing voters.Health information sources also influenced participants’ trust of scientists. Participants who used print and online newspapers, magazines, television, radio, news websites or apps, websites of mainstream organisations, as well as those who obtained information through personal conversations with friends and family or from healthcare environment trust scientists in their countries more than those who do not. Our findings differ from a broader literature on information sources during the COVID-19 pandemic, which have not addressed correlations with trust in scientists.26Participants’ direct experience with COVID-19 (close contact with COVID-19-like symptoms or knowing someone who had been in an ICU), as well as not knowing someone admitted to an ICU for COVID-19, were positively associated with trust in scientists. These apparently contradictory findings, and particularly not knowing someone admitted to an ICU, could have resulted from the large sample size leading to more variables being statistically significant.This study also found that beliefs in conspiracy-related narratives—that the pandemic resulted from a deliberate release of SARS-CoV-2 and that 5G technology exacerbated COVID-19 symptoms—were associated with lower levels of trust in scientists. Similarly, previous studies reported that belief in conspiracy theories was negatively associated with public trust in science27 and adoption of protective behaviours.28 The emergence and circulation of conspiracy narratives (beliefs that ‘major public events are secretly orchestrated by powerful and malevolent entities acting in concert’26) and an infodemic (a plethora of correct and incorrect health information) have been crucial features of this pandemic.20 29 30Our analyses of open-text responses effectively recast our questions about public trust in scientists. First, we found that both respondents trusting and distrusting scientists supported their claims by citing existing scientific research and expressed a need for additional scientific data and research. These results suggest that respondents—even those not trusting national scientists—sought to employ evidence-based thinking. This finding appears to counter claims that those not trusting mainstream scientific discourse act out of emotion or irrationality.15 Although this question requires further investigation, our results suggest that scepticism of existing scientific knowledge on the eve of COVID-19 vaccine rollout in Europe fuelled demands for more scientific evidence. Whereas physicist Edwin Hubble31 argued that ‘a healthy dose of scepticism’ is a prerequisite to scientific thinking, European respondents in this study were highly sceptical of expert judgement. Although Atul Gawande indicates that a scientific mindset ‘observe[s] the world with an open mind, gathering facts and testing […] predictions and expectations against them’,32 distrustful participants in the present study signalled that they undertook similar approaches: they cited published works, they gathered observations, although anecdotal, but ones they considered to be facts. Appropriating this sceptical stance and scientific processes, respondents not trusting mainstream scientists across all surveyed countries suggests a desire to ‘outscience’ the scientists.For Feinstein,33 laypeople are outsiders to science; they rely on scientific knowledge communicated to them. This outsider status uncovers a deep paradox of trust in science: the promise of modern science is to ‘know the truth instead of just trusting what you are told’, and yet trust in science is equally essential, when laypeople cannot surmount barriers of highly specialised, complex scientific knowledge.34 The information revolution once raised hopes for greater public participation in science,19 but new concerns about a post-truth era35 have displaced these earlier aspirations. Still, some respondent efforts to ‘outscience’ the scientists may reflect a continued desire to engage more fully in scientific investigation and findings, to discover truth for themselves. Respondents’ clamours for more data may also result from a conscious strategy to set impossible standards of certainty, to generate doubts and to postpone decision-making about viral origins, vaccines or treatments. Proctor and Schiebinger have described a similar strategy among interest groups engaged in scientific controversies.36Second, our findings raised the question about who can be considered a scientist. Respondents who did not trust scientists in their own countries nevertheless appeared to mention and trust individuals whom they considered to be scientists, but who were controversial or whose status was disputed (eg, Raoult, Trinca). Some commentators have attributed lack of trust in science as the result of ‘fake experts […] who do not actually have a credible scientific track record’.32 Yet, individuals mentioned by respondents—even those roundly castigated by mainstream science for their records during the pandemic—remain difficult to dismiss as ‘fake experts’. Our results highlight the major challenges that the European public face in distinguishing ‘real’ from ‘fake’ scientists. A recent report, for instance, found that 65% of online anti-vaccine content originated with some 12 individuals; our further investigation into these individuals found that half declared that they possessed a medical or biomedical degree.37 The lay public may label active, influential critics as scientists, even when the latter disseminate inaccurate information in their online profiles, are banned from medical boards, or dismissed as pseudo-scientists in news outlets or peer-reviewed journals.Third, we found that the participants’ rationale concerning pandemic origins or plans for COVID-19 treatment or vaccination did not attribute central roles to scientists. Certain respondents appeared to assign more pivotal roles to states, politicians and pharmaceutical companies, suggesting that an intentional viral release would enable powerful actors to reduce certain populations and expenditures on healthcare or social support, or to benefit economically from vaccines. Although these narratives were marked by the absence of scientists, they implied that scientists were nonetheless carrying out agendas of more powerful actors. These results align with Harambam’s findings38 that online Dutch conspiracy narratives often challenge the image of science as a collective, impartial search for knowledge, and that ‘science’, particularly biomedical research, is corrupted by the corporate world.The four principal narratives identified in participants’ justifications for believing in the deliberate release of SARS-CoV-2—demographic control, geopolitical advantage, financial profit and social control—were observed across all countries, languages and cultural areas, although with varying intensities. That these narratives appeared across all country populations included in this survey suggest a shared cultural and linguistic ‘informational ecosystem’ across Europe.Conspiracy narratives, despite their fallacies, offer a window into the underlying anxieties of those believing and spreading them.39 Demographic control narratives were especially prevalent in countries with ageing populations highly affected by COVID-19 in December 2020, notably France, Belgium and Italy. These countries are currently grappling with debates over funding their social retirement systems and sustaining their models of social support. The geopolitical advantage narrative, attributing the pandemic to a Chinese attempt to undermine the West, appeared to resonate with populations anxious about the emergence of a multipolar world, in which Europe and the USA no longer dominate as global economic, cultural and military powers. Respondents from all countries evoked this narrative, but more frequently in Italy and Sweden. Finally, the financial profit and social control narratives, possibly alimented by fears of concentrated power in the hands of private and/or state actors, were somewhat more prominent in France and Italy, which in recent years have been preoccupied by debates over accumulation of wealth and power by these actors.All these narratives often align with and sometimes explicitly reference the Great Reset, a multifaceted conspiracy theory suggesting collusion between governments and large corporations to orchestrate the pandemic.40 Significantly, science and scientists do not feature prominently in such rationale. Scepticism or mistrust of science and scientists does not develop in a vacuum, but is produced and sustained by historical events that shape contemporary attitudes. Past abuses, such as the infamous Tuskegee Syphilis Study in the USA and the Mediator obesity drug scandal, demonstrate that unethical research practices and misapplications of scientific knowledge leave indelible traces on public memory, eroding long-term trust in science and scientists.41–43One singular feature of our study is that it employed an approach that was initially qualitative, then quantitative, then mixed. We first conducted a thematic analysis of online discourse (social listening), using this analysis of the infodemic to inform our survey questions, which integrated key quantitative measures and open-text answers. Quantitatively, we evaluated trust indicators, gauged the prevalence of prominent pandemic conspiracy beliefs, and assessed anticipated vaccine acceptance and treatment preferences. Subsequently, our qualitative analysis highlighted fluid definitions of what constitutes a scientist; the common practice of citing sources to support claims about pandemic origins among both trusting and distrusting participants; four principal themes (demographic control, geopolitical positioning, financial benefit and political control over citizens) that underlay distrustful attitudes towards scientists consistent across nations; and an in-depth mapping of trust dynamics among actors mentioned in participants’ open rationales.Mobilising and combining quantitative and qualitative methodologies leveraged the strengths of each approach. Upstream of the study, qualitative methods crucially highlighted previously unidentified variables through inductive characterisation of online discourse (social listening). These methods also contributed significantly to elucidating and analysing public explanations of their claims around pandemic origins and attitudes towards scientists. In turn, quantitative methods produced additional precision about key indicators of trust in scientists and associated factors and cross-country comparisons of predominant online discourses. Shuttling between and combining mixed-methods appear especially apt for analyses of rapidly changing, polarising and complex subjects like trust in scientists and science during an epidemic or pandemic.Limitations of the studyThis study has multiple limitations. First, because the survey was administered online, respondents with better computer and internet access and higher levels of education were more likely to be recruited and to participate. Moreover, because Ipsos survey panels do not include participants over 65 years old due to uneven internet knowledge and use, we were unable to collect and analyse responses from older populations, which would have been illuminating.Second, the survey was conducted over a 12-day period in December 2020, and in seven European countries. Our results are neither representative of all European countries, nor of high-income countries outside of Europe and middle-income and low-income countries (where populations may be less trustful of scientists). Trust in scientists may have changed significantly since December 2020. For this reason, our findings and conclusions are applicable to the seven European countries where the study was conducted. Although they reveal trust at a specific moment in the past, we employ these results to raise questions implicit in studies of trust in scientists and to encourage further investigation.In investigating factors associated with trust in scientists, the present research did not address trust in science more generally. The survey contained specific questions about scientists’ honestly, integrity and intention to act in the interest of the public. ‘Science’ is a broad term, encompassing multiple actors, processes and practices. We compare our results with studies addressing both trust in ‘scientists’ and ‘science’, although we recognise that these terms do not have the same meaning for respondents.The study’s large (N=7000) sample size in countries with diverse health, political, social, economic and cultural indicators, and conditions led to more statistically significant variables. A study of individual countries could shed additional light on more significant associations.Finally, not all respondents explained their responses in text boxes. It is possible that respondents more adamant about their claims were more likely to respond to these specific questions. That said, in a previous publication, we found that responses to questions about intention to accept COVID-19 vaccination expressed conditionality.44 We would suggest, then, that these responses reflect a broad range of opinions, and not just those more convinced of their claims.ConclusionThis mixed-methods study of trust in scientists study integrated quantitative multivariate analysis and thematic analysis of participants’ open-text rationale. It produced statistically significant results on drivers of trust in scientists among the public in seven European countries, but also identified a shared reliance on evidence-based thinking among participants who trust scientists and those who do not, the relative erasure of scientists from participants’ rationale in favour of other actors and the predominance of controversial scientists among individual scientists.These results should encourage additional investigation of trust in scientists beyond sociodemographic and other drivers, to explore public conceptions of scientists and of scientific investigation. They also should inform multipronged measures to enhance trust in scientists, which should include enhancing scientists’ visibility and emphasising their independence, as well as promoting greater public literacy about scientific investigation and uncertainty. Tackling the broader sociopolitical anxieties about public powerlessness in the face of powerful political and economic interests—which provide fodder for conspiracy narratives—may also indirectly strengthen trust in scientists.Although our findings offer important insight into the dynamics of trust in scientists across selected European countries, they also underscore complexity of this trust. Given its crucial implications for public health policy and communication strategies, more granular investigations of the sociocultural, historical factors influencing public trust at national level are needed. Further research can guide more effective and nuanced science communication in the future.Data availability statementData are available upon reasonable request.Ethics statementsPatient consent for publicationNot required.Ethics approvalThis study involves human participants and the University of Antwerp ethics committee provided ethical approval for all methods of the study, including the initial X (formerly Twitter) analysis (20/13/150). All participants furnished online informed consent before participating in the survey.References↵Mazur A. Public confidence in science. Soc Stud Sci 1977;7:123–5. doi:10.1177/030631277700700113OpenUrlCrossRef↵Gauchat G. Politicization of science in the public sphere: a study of public trust in the United States, 1974 to 2010. Am Sociol Rev 2012;77:167–87. doi:10.1177/0003122412438225OpenUrlCrossRefWeb of Science↵Eurobarometer S. European citizens’ knowledge and attitudes towards science and technology, 4. Eurobarometer, 2021.↵Lewandowsky S, Gignac GE, Oberauer K. The role of conspiracist Ideation and worldviews in predicting rejection of science. PLoS One 2013;8:e75637. doi:10.1371/journal.pone.0075637↵Pechar E, Bernauer T, Mayer F. Beyond political ideology: the impact of attitudes towards government and corporations on trust in science. Sci Commun 2018;40:291–313. doi:10.1177/1075547018763970OpenUrl↵Krimsky S. Science in the private interest: has the lure of profits corrupted biomedical research? Rowman & Littlefield, 2004: 276.↵Bates BR, Harris TM. The Tuskegee study of untreated Syphilis and public perceptions of BIOMEDICAL research: a focus group study. J Natl Med Assoc 2004;96:1051–64.OpenUrlPubMed↵Roundtable on Public Interfaces of the Life SBoard on Life SDivision on Eet al. Trust and confidence at the interfaces of the life sciences and society: does the public trust science? Trust and confidence at the interfaces of the life sciences and society: does the public trust science? A workshop summary. Washington (DC): National Academies Press (US),↵Eiser JR, Stafford T, Henneberry J, et al. "Trust me, I'm a scientist (not a developer)": perceived expertise and motives as predictors of trust in assessment of risk from contaminated land. Risk Anal 2009;29:288–97. doi:10.1111/j.1539-6924.2008.01131.xOpenUrlPubMed↵Algan Y, Cohen D, Davoine E, et al. Trust in scientists in times of pandemic: panel evidence from 12 countries. Proc Natl Acad Sci U S A 2021;118:e2108576118. doi:10.1073/pnas.2108576118↵Bajos N, Spire A, Silberzan L, et al. When lack of trust in the government and in scientists reinforces social inequalities in vaccination against COVID-19. Front Public Health 2022;10:908152. doi:10.3389/fpubh.2022.908152↵Sturgis P, Brunton-Smith I, Jackson J. Trust in science, social consensus and vaccine confidence. Nat Hum Behav 2021;5:1528–34. doi:10.1038/s41562-021-01115-7OpenUrl↵Calleja N, AbdAllah A, Abad N, et al. A public health research agenda for managing Infodemics: methods and results of the first WHO infodemiology conference. JMIR Infodemiology 2021;1:e30979. doi:10.2196/30979↵Bratu S. The fake news sociology of COVID-19 pandemic fear: dangerously inaccurate beliefs, emotional contagion, and conspiracy Ideation. Linguis Philos Invest 2020;19:128. doi:10.22381/LPI19202010OpenUrl↵Magarini FM, Pinelli M, Sinisi A, et al. Irrational beliefs about COVID-19: a scoping review. Int J Environ Res Public Health 2021;18:9839. doi:10.3390/ijerph18199839↵Vranic A, Hromatko I, Tonković M. "I did my own research": overconfidence, (Dis)Trust in science, and endorsement of conspiracy theories. Front Psychol 2022;13:931865. doi:10.3389/fpsyg.2022.931865↵Carrion-Alvarez D, Tijerina-Salina PX. Fake news in COVID-19: a perspective. Health Promot Perspect 2020;10:290–1. doi:10.34172/hpp.2020.44OpenUrl↵Kuhn TS. The structure of scientific revolutions. Chicago: University of Chicago Press, 1962.↵Callon M, Lascoumes P, Barthe Y. Agir Dans UN Monde incertain: Essai sur La Démocratie technique; 2001.↵Eysenbach G. How to fight an Infodemic: the four pillars of Infodemic management. J Med Internet Res 2020;22:e21820. doi:10.2196/21820↵Braun V, Clarke V. Thematic analysis: American psychological association. 2012.↵Wellcome T. Wellcome global monitor 2018: how does the world feel about science and health?; 2019.↵Bromme R, Mede NG, Thomm E, et al. An anchor in troubled times: trust in science before and within the COVID-19 pandemic. PLoS One 2022;17:e0262823. doi:10.1371/journal.pone.0262823↵Lee JJ. Party polarization and trust in science: what about democrats Socius 2021;7:237802312110101. doi:10.1177/23780231211010101OpenUrl↵Allea. Fact or fake? Tackling science disinformation. ALLEA Discussion Paper; 2021. 1–24.↵Chu L, Fung HH, Tse DCK, et al. Obtaining information from different sources matters during the COVID-19 pandemic. Gerontologist 2021;61:187–95. doi:10.1093/geront/gnaa222OpenUrl↵Constantinou M, Kagialis A, Karekla M. COVID-19 scientific facts vs. conspiracy theories: 0 – 1: science fails to convince even highly educated individuals. In Review [Preprint] 2020. doi:10.21203/rs.3.rs-33972/v1↵Winter T, Riordan BC, Scarf D, et al. Conspiracy beliefs and distrust of science predicts reluctance of vaccine uptake of politically right-wing citizens. Vaccine 2022;40:1896–903. doi:10.1016/j.vaccine.2022.01.039OpenUrl↵Bin Naeem S, Kamel Boulos MN. COVID-19 misinformation online and health literacy: a brief overview. Int J Environ Res Public Health 2021;18:8091. doi:10.3390/ijerph18158091↵Antiochou K. Science communication: challenges and dilemmas in the age of COVID-19. Hist Philos Life Sci 2021;43:87. doi:10.1007/s40656-021-00444-0↵Hubble E. The nature of science, and other lectures. Huntington Library, 1954.↵Gawande A. The mistrust of science, the New Yorker 2016. Retrieved; 2021.↵Feinstein N. Salvaging science literacy. Sci Ed 2011;95:168–85. doi:10.1002/sce.20414OpenUrl↵Hendriks F, Kienhues D, Bromme R. Trust in science and the science of trust. Trust and communication in a digitized world: models and concepts of trust research; 2016. 143–59.↵Higgins K. Post-truth: a guide for the perplexed. Nature 2016;540:9. doi:10.1038/540009a↵Proctor RN, Schiebinger L. Agnotology: the making and unmaking of ignorance. California: Stanford University Press Stanford, 2008.↵Center for Countering Digital Hate. The Disinformation dozen 2021; 2021.↵Harambam J. Contemporary conspiracy culture: truth and knowledge in an era of epistemic instability. Routledge, 2020.↵Morin E. Rumor in Orleans. New York: Pantheon, 1971.↵Christensen M, Anson A. The great reset and the cultural boundaries of conspiracy theory. Int J Commun 2023;17:19.OpenUrl↵Lederer S, Davis AB. Subjected to science: human experimentation in America before the second World War. History: Reviews of New Books 1995;24:13. doi:10.1080/03612759.1995.9949143OpenUrl↵Frachon I. Médiator 150 mg: Combien de morts?: Éditions dialogues; 2010. 2010.↵Reverby SM. Examining tuskegee: The infamous syphilis study and its legacy. Univ of North Carolina Press, 2009.↵Heyerdahl LW, Vray M, Lana B, et al. Conditionality of COVID-19 vaccine acceptance in European countries. Vaccine 2022;40:1191–7. doi:10.1016/j.vaccine.2022.01.054OpenUrl
|
|
Scooped by
Gilbert C FAURE
October 23, 2023 11:11 AM
|
The recent health crisis and the rapid development of Artificial Intelligence have caused misinformation on social media to flourish by becoming more sophisticated and challenging to detect. This calls upon fact-checking and questions users’ competencies and attitudes when assessing social media...
|
|
Scooped by
Gilbert C FAURE
August 20, 2023 3:53 AM
|
COVID-19 vaccines are an effective public health intervention to reduce COVID-19-related morbidity and mortality. Given that pregnant and lactating women have a higher risk of severe COVID-19 complications, it is paramount to understand the factors that inform vaccine decision-making among this...
|
|
Scooped by
Gilbert C FAURE
July 20, 2023 5:58 AM
|
Widespread vaccination against important diseases plays a key role for global health security, particularly in the context of the COVID-19 pandemic. However, building and maintaining trust in immunization services remains challenging because of doubts about quality and safety of vaccines.
|
|
Rescooped by
Gilbert C FAURE
from veille vaccination
March 3, 2023 5:24 AM
|
Read the latest articles of Pediatric Clinics of North America at ScienceDirect.com, Elsevier’s leading platform of peer-reviewed scholarly literature
Via HAS-veille
|
|
Scooped by
Gilbert C FAURE
October 18, 2022 7:06 AM
|
COVID-19 vaccine acceptance depends on the characteristics of new vaccines and the
national vaccination strategy, among various other factors, in the working-age population
in France.
|
|
Rescooped by
Gilbert C FAURE
from Wuhan, Hubei
May 25, 2022 10:58 AM
|
Background COVID-19 vaccine has been available in China since the beginning of the 2021, however, certain numbers of people are reluctant for some reasons to vaccinate. The high vaccine coverage is crucial for controlling disease transmission, however, the vaccine hesitancy might be a barrier to the establishment of sufficient herd immunization. This study aims to investigate the prevalence of the COVID-19 vaccine hesitancy among different population groups, and explore common barriers and facilitators to vaccination decisions. Methods The current survey was performed among Chinese students, public health professionals, medical workers and general population from January to March 2021 from seven cities in China. The questionnaire contained sociodemographic information, concerns about infection with COVID-19, general vaccination behaviors and attitudes, the General Vaccine Hesitancy Scale, the COVID-19 Vaccine Hesitancy Scale and other potential factors. Univariate analysis was conducted by chi-squared test, and variables significant at P < 0.10 were then included in a multivariable regression model. Results The prevalence of COVID-19 vaccine hesitancy was 15.6% in our study, and 23.9% of students, 21.2% of the general population, 13.1% of medical workers, and 10.4% of public health professionals had vaccine hesitancy. The results of multivariate analysis indicated that participants who had received negative information of COVID-19 vaccine (OR: 1.563, 95% CI: 1.229–1.986) and who had doubts about the information source (OR: 2.157, 95% CI: 1.697–2.742) were more likely to have vaccine hesitancy. While those who needed transparent information about COVID-19 vaccine (OR: 0.722, 95% CI: 0.535–0.973) and who would get COVID-19 vaccine if doctors recommended (OR: 0.176, 95% CI: 0.132–0.234) were less likely to have COVID-19 vaccine hesitancy. Conclusions Given recommendations from medical workers about vaccination can motivate people to accept COVID-19 vaccination, appropriate training in knowledge about vaccines and communication skills are necessary for them to increase public’s willingness of vaccination. Reducing the spread of misinformation and disseminating facts in a timely and accurate way will likely reduce vaccine hesitancy. Moreover, to establish suitable communication strategies and information exchange platforms between the government and the public and a warning system on infodemic would be helpful to improve public’s confidence in vaccination.
|
|
Scooped by
Gilbert C FAURE
May 6, 2022 2:45 PM
|
The use of social media has increased substantially over the past decade, which has also created many new opportunities for research. Social networks can be used for research planning, recruitment of specific populations to research studies, and dissemination of results. In addition, many studies have used social media as a source of observational data or a platform within which to conduct experimental studies. Some studies have leveraged social media to study other issues such as cancer survivorship, whereas in other studies, the research question is about social media itself.ChooseTop of page <<REFERENCESUse of Social Media for Research InitiationBeginning with the initial stages of the research process, social media are extremely useful to identify patient priorities for research and recruit participants. For example, posts from an online health community were used to generate comparative effectiveness research questions about bladder cancer.1 Another study used Twitter and other social networks to recruit breast cancer survivors to take a survey about lifestyle changes after diagnosis.2 These examples highlight a few ways that social media can help develop patient-centered research design and facilitate targeted recruitment efforts.Observational Studies Using Social MediaThe data from social media are often used in oncology research, including content analysis using qualitative and/or quantitative methods. Content analysis of social media data has provided a valuable source of information on public perceptions and unmet needs of patients with cancer and their families.Qualitative analysis.Qualitative analysis of online content, such as forum posts, can offer unique insights into the lived experience with cancer because of the presence of large global communities of patients and their families on social media. For example, we recently examined data from an online health community about prostate cancer to examine its impact on sexual health for partners of patients, an understudied issue in survivorship care.3 Another example is the use of Twitter to identify barriers to care in patients with metastatic breast cancer.4 The results of this research are an important contribution to advance patient care and policy initiatives.Meanwhile, it is also extremely important for health care providers to be aware of the type of information that patients and their families are seeing on social media. To this end, many studies have performed qualitative analysis of the quality of social media content about various cancer topics. These studies often incorporate manual review of social media posts by experts to identify the quality of content shared on social media platforms, using validated instruments such as the DISCERN criteria and Patient Education Materials Assessment Tools,5,6 and the presence of commercial bias and misinformation.7Misinformation.Many studies have revealed the dark side of social media in enabling the broad dissemination of poor-quality and misinformative content. A content analysis of publicly available Facebook pages hosted by parents of children with acute lymphoblastic leukemia reported that 19% of the information was not medically/scientifically accurate and 14% described unproven treatment modalities.8 Our group manually reviewed the top 150 YouTube videos in a search for “prostate cancer,” demonstrating a substantial amount of biased and potentially misinformative content.7 We found similar results in analysis of YouTube videos about other urological cancers (eg, bladder cancer)9 and analysis of prostate cancer content on other social networks (eg, TikTok).10 A separate study found that inaccurate and misleading articles about genitourinary cancer are more likely to be shared on social media.11Representation of diversity.In addition to the accuracy of the information being shared, another critical consideration is the representation of diversity in online content about cancer, which may play a role in health disparities. We recently examined the perceived racial and ethnic diversity of people in YouTube videos and websites about prostate cancer through a consensus process including community stakeholders.12 The results showed underrepresentation of Black and Hispanic people in online content about prostate cancer, despite a higher risk of aggressive prostate cancer in these men. We are currently studying the impact of online information on health disparities in prostate cancer. Overall, the results from this type of social media research provide important data on the gaps in currently available online content about cancer. This is essential to inform the development of new content that is accurate, understandable, and inclusive. This body of social media research also highlights the importance of health care providers taking an active approach in disseminating high-quality content to their patients and the general public.Quantitative analysis.Multiple studies have applied a quantitative approach to social media data analysis, including comparisons of social media activity between different cancers, time periods, or in relation to temporal events. For example, we reported less Twitter activity13 and fewer donations through crowdfunding sites14 for prostate cancer compared with breast cancer. More recently, we found substantially less engagement on Twitter, Facebook, and YouTube about BRCA and genetic testing in prostate cancer compared with breast cancer.15 These analyses can provide insights into public awareness about different topics and potential strategies for health communication campaigns.Mixed methods approach.In addition, some studies in oncology have leveraged a mixed methods approach, including qualitative and quantitative methods. For example, we examined posts to an online prostate cancer community that mentioned sleep.16 Qualitative analysis revealed that sleeping problems presented a significant impairment to quality of life among patients with prostate cancer. Quantitative analysis using linguistic inquiry word count revealed greater negative emotion in posts regarding sleep by patients with advanced compared with localized prostate cancer, suggesting that this population is an important target for sleep health promotion. Overall, a combination of qualitative and quantitative approaches can increase scientific rigor and provide new insights beyond either approach alone.Experimental Studies Using Social MediaSocial media have also been used for interventional studies. Analogous to the observational studies described above, some of these studies used social media to deliver an intervention designed for a specific outcome (eg, quality of life) while others were designed to study social media behavior in response to an intervention. For example, a study of continence rates in patients after radical prostatectomy found that providing guidance for pelvic floor exercises through WeChat along with standard education about pelvic floor exercises was associated with better continence compared with exercises alone.17 Another study looked at the impact of user exposure to educational videos on evaluating news literacy and debunking scrolling comments on their ability to identify sunscreen misinformation related to skin cancer in Facebook videos.18Use of Social Media for Research DisseminationSocial media have become an essential part of research dissemination within the scientific community and to the general public. Studies have shown the expansion in social media use at oncology conferences, allowing broader audiences to follow the latest scientific developments.19 Social media have also been used for dissemination of clinical practice guidelines and to conduct journal clubs.20 For example, the Twitter-based prostate cancer journal club (indexed using the hashtag #prostatejc) discusses important new publications with a global, multidisciplinary audience.21Future DirectionsDespite a substantial amount of research using social media in oncology, there are important gaps for future study. One important direction for future research is greater characterization of the long-term efforts of social media communications on clinical decision making and well-being in patients with cancer. The impact of social media information on health disparities is also an important area for future study. Studies are needed to determine whether exposure to online misinformation leads to worse health outcomes, whether automated solutions (eg, using machine learning algorithms) could be used to help identify misinformative content, and what are the best strategies to combat misinformation.From a methodologic standpoint, there are challenges in applying validated instruments in health communications (such as DISCERN) to the vastly different types of social media content.10 Continued development of methods and instruments for use in social media research is an important future direction. This includes the adaptation of frameworks to characterize the effects of social media in oncology22 and standardized reporting criteria to ensure scientific rigor in social media research.23In conclusion, social networks can be used at every stage of the research process, including planning and recruitment, a source of data, and dissemination of results to large audiences. Research about social media has highlighted its potential value to raise awareness, provide public education, and highlight unmet needs of patients and their families; however, there are also major concerns with representativeness and quality of online content. More research is needed into the downstream impact of social media in oncology, as well as optimal strategies to combat misinformation on social networks.© 2022 by American Society of Clinical OncologySUPPORTSL is supported by the Department of Defense, Prostate Cancer Foundation, and the Edward Blank and Sharon Cosloy-Blank Family Foundation.AUTHOR CONTRIBUTIONSConception and design: All authorsAdministrative support: All authorsCollection and assembly of data: All authorsData analysis and interpretation: All authorsManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authorsAUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTERESTMethodologies in Social Media Research: Where We Are and Where We Still Need to Go?The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/op/authors/author-center.Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).Stacy LoebStock and Other Ownership Interests: Gilead Sciences (I)Rena MalikHonoraria: MedtronicSpeakers' Bureau: Urovant SciencesOpen Payments Link: https://openpaymentsdata.cms.gov/physician/976042No other potential conflicts of interest were reported.REFERENCESChooseTop of pageREFERENCES <<1. Mossanen M, Chu A, Smith AB, et al: Inferring bladder cancer research prioritization from patient-generated online content. World J Urol 37:1145-1150, 2019 Crossref, Medline, Google Scholar2. Keaver L, McGough AM, Du M, et al: Self-reported changes and perceived barriers to healthy eating and physical activity among global breast cancer survivors: Results from an exploratory online novel survey. J Acad Nutr Diet 121:233-241.e8, 2021 Crossref, Medline, Google Scholar3. Loeb SS, Nelson CJ, Mulhall JP, et al: Comparison of Sexual Concerns Between Patients With Prostate Cancer and Their Partners. Scottsdale, AZ, Sexual Medicine Society of North America, 2021 Google Scholar4. Shimkhada R, Attai D, Scheitler AJ, et al: Using a Twitter chat to rapidly identify barriers and policy solutions for metastatic breast cancer care: Qualitative study. JMIR Public Health Surveill 7:e23178, 2021 Crossref, Medline, Google Scholar5. DISCERN Quality Criteria for Consumer Health Information. http://www.discern.org.uk/discern_instrument.php Google Scholar6. AHRQ: The Patient Education Materials Assessment Tool (PEMAT) and User's Guide. https://www.ahrq.gov/professionals/prevention-chronic-care/improve/self-mgmt/pemat/pemat-av.html Google Scholar7. Loeb S, Sengupta S, Butaney M, et al: Dissemination of misinformative and biased information about prostate cancer on YouTube. Eur Urol 75:564-567, 2019 Crossref, Medline, Google Scholar8. Gage-Bouchard EA, LaValley S, Warunek M, et al: Is cancer information exchanged on social media scientifically accurate? J Cancer Educ 33:1328-1332, 2018 Crossref, Medline, Google Scholar9. Loeb S, Reines K, Abu-Salha Y, et al: Quality of bladder cancer information on YouTube. Eur Urol 79:56-59, 2021 Crossref, Medline, Google Scholar10. Xu AJ, Taylor J, Gao T, et al: TikTok and prostate cancer: Misinformation and quality of information using validated questionnaires. BJU Int 128:435-437, 2021 Crossref, Medline, Google Scholar11. Alsyouf M, Stokes P, Hur D, et al: “Fake news” in urology: Evaluating the accuracy of articles shared on social media in genitourinary malignancies. BJU Int 10.1111/bju.14787 [epub ahead of print on May 2, 2019] Google Scholar12. Loeb SB HT, Gomez S, Ravenell J, et al: Representation in online prostate cancer content lacks racial and ethnic diversity: Implications for Black and Latinx men. J Urol 207:559-564, 2022 Crossref, Medline, Google Scholar13. Loeb S, Stork B, Gold HT, et al: Tweet this: How advocacy for breast and prostate cancers stacks up on social media. BJU Int 120:461-463, 2017 Crossref, Medline, Google Scholar14. Loeb S, Taneja S, Walter D, et al: Crowdfunding for prostate cancer and breast cancer. BJU Int 122:723-725, 2018 Crossref, Medline, Google Scholar15. Loeb S, Massey P, Leader AE, et al: Gaps in public awareness of BRCA and genetic testing in prostate cancer: A social media landscape analysis. JMIR Cancer 7:e27063, 2021 Crossref, Medline, Google Scholar16. Robbins R, Jean-Louis G, Chanko N, et al: Using data from an online health community to examine the impact of prostate cancer on sleep. BJU Int 125:634-635, 2020 Crossref, Medline, Google Scholar17. Junwen S, Rongjiang W: The efficacy of the WeChat app combined with pelvic floor muscle exercise for the urinary incontinence after radical prostatectomy. Biomed Res Int 2020:6947839, 2020 Crossref, Medline, Google Scholar18. Vraga EK, Bode L, Tully M: The effects of a news literacy video and real-time corrections to video misinformation related to sunscreen and skin cancer. Health Commun 1-9, 2021 Crossref, Medline, Google Scholar19. Pemmaraju N, Thompson MA, Mesa RA, et al: Analysis of the use and impact of twitter during American Society of Clinical Oncology annual meetings from 2011 to 2016: Focus on advanced metrics and user trends. J Oncol Pract 13:e623-e631, 2017 Link, Google Scholar20. Bhatt NR, Czarniecki SW, Borgmann H, et al: A systematic review of the use of social media for dissemination of clinical practice guidelines. Eur Urol Focus 7:1195-1204, 2021 Crossref, Medline, Google Scholar21. Loeb S, Taylor J, Butaney M, et al: Twitter-based prostate cancer journal club (#ProstateJC) promotes multidisciplinary global scientific discussion and research dissemination. Eur Urol 75:881-882, 2019 Crossref, Medline, Google Scholar22. Schillinger D, Chittamuru D, Ramirez AS: From “infodemics” to health promotion: A novel framework for the role of social media in public health. Am J Public Health 110:1393-1396, 2020 Crossref, Medline, Google Scholar23. Roland D, Spurr J, Cabrera D: Initial standardized framework for reporting social media analytics in emergency care research. West J Emerg Med 19:701-706, 2018 Crossref, Medline, Google Scholar
|
|
Scooped by
Gilbert C FAURE
April 19, 2022 3:28 AM
|
|
|
Scooped by
Gilbert C FAURE
March 14, 2022 12:03 PM
|
2 articles importants publiés le 10/03 dans Nature Portfolio qui permettent une meilleure compréhension de la désinformation médicale et des théorie
|
|
Scooped by
Gilbert C FAURE
August 2, 2021 3:03 AM
|
Identifying and understanding COVID-19 vaccine hesitancy within distinct populations may aid future public health messaging. Using nationally representative data from the general adult populations of Ireland (N = 1041) and the United Kingdom (UK; N = 2025), we found that vaccine hesitancy/resistance was evident for 35% and 31% of these populations respectively. Vaccine hesitant/resistant respondents in Ireland and the UK differed on a number of sociodemographic and health-related variables but were similar across a broad array of psychological constructs. In both populations, those resistant to a COVID-19 vaccine were less likely to obtain information about the pandemic from traditional and authoritative sources and had similar levels of mistrust in these sources compared to vaccine accepting respondents. Given the geographical proximity and socio-economic similarity of the populations studied, it is not possible to generalize findings to other populations, however, the methodology employed here may be useful to those wishing to understand COVID-19 vaccine hesitancy elsewhere. Hesitancy and resistance towards vaccination is a challenge for public health. Here the authors determine psychological characteristics associated with COVID-19 vaccine hesitancy or resistance attitudes in the UK and Ireland.
|