Your new post is loading...
Your new post is loading...
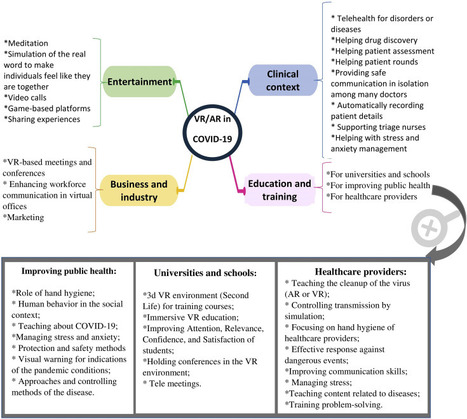
The pandemics of major infectious diseases often cause public health, economic, and social problems. Virtual reality (VR) and augmented reality (AR), as two novel technologies, have been used in many fields for emergency management of disasters. The objective of this paper was to review VR and AR applications in the emergency management of infectious outbreaks with an emphasis on the COVID-19 outbreak. It appears that VR and AR technologies can play a positive role during infectious disease outbreaks. VR and AR have been widely used in the prevention and response phases of emergency management during infectious disease pandemics, such as SARS and Ebola pandemics, especially for educating and training purposes for the public. During the COVID-19 outbreak, these technologies have the potential to be used in various fields, including 1) clinical context (e.g., telehealth, drug discovery, patient assessment, mental health management), 2) entertainment (e.g., video call, meditation, gaming), 3) business and industry (e.g., holding meetings and conferences, marketing), and 4) education (e.g., in schools and universities, for healthcare providers, and VR-based content for improving public health). These technologies can be used in the above-mentioned fields by providing their different features for facilitating the challenges of COVID-19. However, to respond to COVID-19, all applications of VR and AR should be considered as a supportive approach alongside other information technologies. We believe that VR and AR have a substantial potential to impact the emergency management of COVID-19 or any infectious disease pandemics; however, these potentials need to be studied in a more robust manner. read the paper ta https://www.sciencedirect.com/science/article/pii/S2352914821000691

|
Scooped by
nrip
|
The COVID-19 pandemic is the greatest public health crisis of the last 100 years. Countries have responded with various levels of lockdown to save lives and stop health systems from being overwhelmed. At the same time, lockdowns entail large socioeconomic costs. One exit strategy under consideration is a mobile phone app that traces the close contacts of those infected with COVID-19. Recent research has demonstrated the theoretical effectiveness of this solution in different disease settings. However, concerns have been raised about such apps because of the potential privacy implications. This could limit the acceptability of app-based contact tracing in the general population. As the effectiveness of this approach increases strongly with app uptake, it is crucial to understand public support for this intervention. Objective: The objective of this study is to investigate the user acceptability of a contact-tracing app in five countries hit by the pandemic.
Methods: We conducted a largescale, multicountry study (N=5995) to measure public support for the digital contact tracing of COVID-19 infections.
We ran anonymous online surveys in France, Germany, Italy, the United Kingdom, and the United States and measured intentions to use a contact-tracing app across different installation regimes (voluntary installation vs automatic installation by mobile phone providers) and studied how these intentions vary across individuals and countries.
Results: We found strong support for the app under both regimes, in all countries, across all subgroups of the population, and irrespective of regional-level COVID-19 mortality rates.
We investigated the main factors that may hinder or facilitate uptake and found that concerns about cybersecurity and privacy, together with a lack of trust in the government, are the main barriers to adoption.
Conclusions:
Epidemiological evidence shows that app-based contact tracing can suppress the spread of COVID-19 if a high enough proportion of the population uses the app and that it can still reduce the number of infections if uptake is moderate. Our findings show that the willingness to install the app is very high. The available evidence suggests that app-based contact tracing may be a viable approach to control the diffusion of COVID-19. read the study at https://mhealth.jmir.org/2020/8/e19857
|
|
Scooped by
nrip
|
Since the start of the pandemic, new technologies have been developed to help reduce the spread of the infection. Some of the most common safety measures today include measuring a person’s temperature, covering your nose and mouth with a mask, contact tracing, disinfection, and social distancing. Many businesses have adopted various technologies, including those with artificial intelligence (AI) underneath, helping to adhere to the COVID-19 safety measures. As an example, numerous airlines, hotels, subways, shopping malls, and other institutions are already using thermal cameras to measure an individual’s temperature before people are allowed entry. In its turn, public transport in France relies on AI-based surveillance cameras to monitor whether or not people are social-distancing or wearing masks. Another example is requiring the download of contact-tracing apps delivered by governments across the globe. However, there are a number of issues. While many of these solutions help to ensure that COVID-19 prevention practices are observed, many of them have flaws or limits. In this article, we will cover some of the issues creating obstacles for fighting the pandemic. Issue #1. Manual temperature scanning is tricky Issue #2. Monitoring crowds is even more complex Issue #3. Contact tracing leads to privacy concerns Issue #4. UV rays harm eyes and skin Issue #5. UVC robots are extremely expensive Issue #6. No integration, no compliance, no transparency Regardless of the safety measures in place and existing issues, innovations are already playing a vital role in the fight against COVID-19. By improving on existing technology, we can make everyone safer as we all adjust to the new normal. read the details at https://www.altoros.com/blog/whats-wrong-with-ai-tools-and-devices-preventing-covid-19/
|
|
Scooped by
nrip
|
The enormous pressure of the increasing case numbers experienced during the COVID-19 pandemic has given rise to a variety of novel digital systems designed to provide solutions to unprecedented challenges in public health. The field of algorithmic contact tracing, in particular, an area of research that had previously received limited attention, has moved into the spotlight as a crucial factor in containing the pandemic. The use of digital tools to enable more robust and expedited contact tracing and notification, while maintaining privacy and trust in the data generated, is viewed as key to identifying chains of transmission and close contacts, and, consequently, to enabling effective case investigations. Scaling these tools has never been more critical, as global case numbers have exceeded 100 million, as many asymptomatic patients remain undetected, and as COVID-19 variants begin to emerge around the world. In this context, there is increasing attention on blockchain technology as a part of systems for enhanced digital algorithmic contact tracing and reporting. By analyzing the literature that has emerged from this trend, the common characteristics of the designs proposed become apparent. An archetypal system architecture can be derived, taking these characteristics into consideration. However, assessing the utility of this architecture using a recognized evaluation framework shows that the added benefits and features of blockchain technology do not provide significant advantages over conventional centralized systems for algorithmic contact tracing and reporting. From our study, it, therefore, seems that blockchain technology may provide a more significant benefit in other areas of public health beyond contact tracing. more at https://publichealth.jmir.org/2021/4/e26460
|
|
Scooped by
nrip
|
Vaccination Passports - What are they?
As mass vaccination programs are being rolled out globally, vaccine passports have become a major topic of discussion. COVID test results and proof of vaccine will be required in many countries for quarantine-free travel, just as it has been for polio and yellow fever vaccinations in the past. Countries will need to look at convenient and secure ways for verifying COVID-19 test results and vaccination information at airports and borders. The International Air Transport Association (IATA) has also called for a “global standard to securely record digital proof of vaccination”. They have been promoting the IATA Travel Pass Initiative (https://www.iata.org/en/programs/passenger/travel-pass/) In February, Qantas completed a trial run of an app for this purpose on an international repatriation flight from Frankfurt to Darwin. The idea behind the app is that health or border officials and airline staff may be able to easily verify COVID-19 test results and vaccination history of an individual. The app links customers with certified testing labs to allow their results to be automatically uploaded onto it. Similar digital solutions are being developed in several other countries around the world to enable travel again. For instance, travellers from Singapore will receive a notarized certificate following a negative COVID-19 test that they can present at airports around the world. Another example is France taking part in a month-long trial of a vaccine passport that leverages a smart phone app. Its important that such digital health technologies, whether apps or chip cards, or health tracker add ons, be easy to use. It important that the process be as seamless as possible for flyers share the relevant information as well as get the information validated by the ground and air staff so they people can travel internationally, again, safely! image source: https://foto.wuestenigel.com/person-hands-holding-a-covid-19-passport/ image license: https://creativecommons.org/licenses/by/2.0/
|
|
Scooped by
nrip
|
We are directionally headed towards a significant shift in the way care is delivered. The rapid up scaling of virtual care capacity and the mainstreaming of Telehealth have given rise to new digital health tools. Self-triaging and contact tracing for COVID-19 infection detection are among the new breed of digital health applications that startups to big firms alike were looking at to seize the emerging opportunities. Telehealth is here to stay. Healthcare is shifting to virtual care models. Digital front door apps are all the rage. What else is emerging that could change the way we experience care? While telehealth is now the de facto mode of accessing healthcare for most low-acuity and routine care needs, a number of related technology-led trends are quietly gaining ground as well. Here the author looks at a few of these and opinionates on their potential impact on healthcare consumer experiences. "contactless" experiences: Covid has made us all afraid to touch any surface exposed to the public. Nowhere is this fear more prominent than a hospital or clinic setting. Healthcare executives now speak of airport check-in type of experiences for healthcare appointments, both for in-person and virtual visits. Technology-enabled workflows now enable patients to complete most of the registration formalities prior to the visit, be it a virtual consult or a clinic visit. Registration kiosks in hospital lobbies may soon be enabled with facial recognition software to eliminate the need for touching any surface. Routine examinations are also going virtual, with many diagnostic procedures now possible through remotely controlled devices. Caregivers are beginning to do their patient rounds through virtual visits. This trend will only grow in the coming years. Contact tracing Inspired by the success of India, Singapore and South Korea, contact tracing applications on Bluetooth-enabled devices have been positioned as an effective means to track and trace infections to reduce the spread of COVID-19 Despite many setbacks, contact tracing's potential for deployment within communities and populations for uses beyond COVID-19 has longer-term potential, and this could be the single most important technology-enabled healthcare program to come out of the COVID-19 crisis. Remote monitoring and automated communication Healthcare executives are more motivated than ever to keep their populations healthy in their homes. A vast and growing array of automated communication tools allows caregivers to use rule-based messaging to push everything from health coaching, post-discharge care instructions, and appointment reminders through IVR, text, SMS, and mobile alerts. Data mining tools can identify subsets of populations at risk and enable caregivers to intervene on time. A New York-based COVID-19 Rapid Response Coalition involving tech giant Amazon that targeted high-risk populations through SMS campaigns that reached up to 10,000 members a day, is an example of how automated communication tools can serve populations in a crisis and during normal times. The use of digital health and automated communication tools has also improved healthcare outcomes by reducing no-shows for appointments, increased adherence to medication regimens, and targeted interventions during adverse events. There is an unprecedented opportunity today to use telehealth technologies in the complete continuum of care. However, healthcare enterprises and their technology partners need to make them more user-friendly. That will determine success for new technology-enabled virtual care models. Every health system has to design the digital experience that is suited for their patient populations while remembering to address the needs of caregivers who will deliver and manage the experiences.
|
|
|
Scooped by
nrip
|
While the US debates the value of the modality, a South Korean survey finds that patients like to use audio-only telehealth platforms to connect with their care provider - but their providers aren’t so sure. While telehealth is not legally allowed in South Korea, the Ministry of Health and Welfare temporarily permitted its use due to hospital closures at the start of the pandemic. Between February 24 and March 7, 2020, 6,840 patients used audio-based telehealth. Researchers sent surveys to patients and providers alike to gauge their satisfaction with the telehealth platform, which includes landline telephones and online services without video. They asked questions about ease-of-use, interaction quality, reliability, satisfaction, and future use. Around 87 % of patients reported that they were satisfied with their provider interaction and felt they could effectively express their feelings during an audio-only telehealth visit. Most patients (87.1 %) also responded that their telehealth visit was just as reliable as an in-person visit would have been. Meanwhile, the providers’ opinions differed drastically. Less than 10 % of doctors and nurses were satisfied with their ability to interact with patients through an audio-only telehealth visit compared to in-person visits (7.3 % and 9 %, respectively). Only 14 % of providers felt that the visits were as reliable as an in-person visit. Patients and providers also had differing opinions on the convenience of telehealth. Nearly 80 % of patients were satisfied with the convenience of telehealth and found it easy to use. Providers were not as satisfied, with only 38.2 % of doctors and 30 percent of nurses reporting that they found telehealth convenient. Overall, providers felt the negatives outweighed the positives for audio-only telehealth. While 85.8 % of the doctors and nurses agreed that telehealth is appropriate for emergency situations such as a pandemic, only 27.7 said it would be appropriate at all times. In contrast, 40 % of the doctors and nurses surveyed said telehealth would be appropriate if it involved an audio-visual platform, saying it would be easier to fully examine and diagnose a patient’s condition. read more at https://mhealthintelligence.com/news/audio-only-telehealth-has-its-fans-patients-and-its-critics-providers
|
|
Scooped by
nrip
|
The COVID-19 pandemic has had an unprecedented impact on the education and wellbeing of medical trainees. In supporting learning during these times, residency programs have adopted flexible scheduling, focused on frequent and transparent communication, incorporated different strategies to build community and promote psychological wellbeing, and advanced virtual teaching modalities. We are hopeful that these interventions will be long lasting. This pandemic will undoubtedly be a defining moment in our careers and our lives. We not only learned to be better physicians; the experience has made us better human beings. We shared the same fears and worries of our patients and their families and became more compassionate; we grew more patient, flexible and understanding. We were taught important lessons in courage and teamwork. From this experience, we have learned not to fear the unknown, but to grow from the process and rebuild stronger. The aim of this article is to share strategies that have helped us to move forward in the aftermath of the first phases of the pandemic, whilst we prepare for the uncertainty of the future. We hope that the lessons we have learned can help inform other programs as they react and adapt to the global after-effects of this crisis. The - Prioritize Residents' Wellbeing
- Incorporate Leadership Training into the Curriculum
- Establish Frequent and Active Communication
- Continue to Build Community – Even Virtually
- Embrace Technology
- Every Day, Small Gestures Can Have a Large Impact
read the entire paper at https://www.dovepress.com/rebuilding-graduate-medical-education-after-a-crisis-perspectives-of-m-peer-reviewed-fulltext-article-AMEP
|
|
Scooped by
nrip
|
Contact tracing apps are potentially useful tools for supporting national COVID-19 containment strategies. Various national apps with different technical design features have been commissioned and issued by governments worldwide.
Objective: Our goal was to develop and propose an item set that was suitable for describing and monitoring nationally issued COVID-19 contact tracing apps.
This item set could provide a framework for describing the key technical features of such apps and monitoring their use based on widely available information.
Methods: We used an open-source intelligence approach (OSINT) to access a multitude of publicly available sources and collect data and information regarding the development and use of contact tracing apps in different countries over several months (from June 2020 to January 2021). The collected documents were then iteratively analyzed via content analysis methods. During this process, an initial set of subject areas were refined into categories for evaluation (ie, coherent topics), which were then examined for individual features.
These features were paraphrased as items in the form of questions and applied to information materials from a sample of countries (ie, Brazil, China, Finland, France, Germany, Italy, Singapore, South Korea, Spain, and the United Kingdom [England and Wales]). This sample was purposefully selected; our intention was to include the apps of different countries from around the world and to propose a valid item set that can be relatively easily applied by using an OSINT approach.
Results: Our OSINT approach and subsequent analysis of the collected documents resulted in the definition of the following five main categories and associated subcategories:
(1) background information (open-source code, public information, and collaborators); (2) purpose and workflow (secondary data use and warning process design); (3) technical information (protocol, tracing technology, exposure notification system, and interoperability); (4) privacy protection (the entity of trust and anonymity); and (5) availability and use (release date and the number of downloads). Based on this structure, a set of items that constituted the evaluation framework were specified. The application of these items to the 10 selected countries revealed differences, especially with regard to the centralization of the entity of trust and the overall transparency of the apps’ technical makeup.
Conclusions: We provide a set of criteria for monitoring and evaluating COVID-19 tracing apps that can be easily applied to publicly issued information. The application of these criteria might help governments to identify design features that promote the successful, widespread adoption of COVID-19 tracing apps among target populations and across national boundaries.
read the study at https://mhealth.jmir.org/2021/3/e27232
|
|
Scooped by
nrip
|
Web-based technology has dramatically improved our ability to detect communicable disease outbreaks, with the potential to reduce morbidity and mortality because of swift public health action. Apps accessible through the internet and on mobile devices create an opportunity to enhance our traditional indicator-based surveillance systems, which have high specificity but issues with timeliness.
Objective: The aim of this study is to describe the literature on web-based apps for indicator-based surveillance and response to acute communicable disease outbreaks in the community with regard to their design, implementation, and evaluation.
Results: Apps were primarily designed to improve the early detection of disease outbreaks, targeted government settings, and comprised either complex algorithmic or statistical outbreak detection mechanisms or both.
We identified a need for these apps to have more features to support secure information exchange and outbreak response actions, with a focus on outbreak verification processes and staff and resources to support app operations. Conclusions: Public health officials designing new or improving existing disease outbreak web-based apps should ensure that outbreak detection is automatic and signals are verified by users, the app is easy to use, and staff and resources are available to support the operations of the app and conduct rigorous and holistic evaluations. read the study at https://publichealth.jmir.org/2021/4/e24330
|
|
Scooped by
nrip
|
With cases soaring across the globe, the Covid-19 pandemic is nowhere near its end, but with three vaccines reporting trial data and two apparently nearing approval by the US FDA, it may be reaching a pivot point. In what feels like a moment of drawing breath and taking stock, international researchers are turning their attention from the present back to the start of the pandemic, aiming to untangle its origin and asking what lessons can be learned to keep this from happening again. Two efforts are happening in parallel. On November 5, the World Health Organization quietly published the rules of engagement for a long-planned and months-delayed mission that creates a multinational team of researchers who will pursue how the virus leaped species. Meanwhile, last week, a commission created by The Lancet and headed by the economist and policy expert Jeffrey Sachs announced the formation of its own international effort, a task force of 12 experts from nine countries who will undertake similar tasks. Both groups will face the same complex problems. It has been approximately a year since the first cases of a pneumonia of unknown origin appeared in Wuhan, China, and about 11 months since the pneumonia’s cause was identified as a novel coronavirus, probably originating in bats. The experts will have to retrace a chain of transmission—one or multiple leaps of the virus from the animal world into humans—using interviews, stored biological samples, lab assays, environmental surveys, genomic data, and the thousands of papers published since the pandemic began, all while following a trail that may have gone cold. The point is not to look for patient zero, the first person infected—or even a hypothetical bat zero, the single animal from which the novel virus jumped. It’s likely neither of those will ever be found. The goal instead is to elucidate the ecosystem—physical, but also viral—in which the spillover happened and ask what could make it likely to happen again. more at WIRED : https://www.wired.com/story/two-global-efforts-try-to-trace-the-origin-of-the-covid-virus/?utm_source=pocket-newtab-intl-en
|
|
Scooped by
nrip
|
With fear of COVID-19 keeping many routine visitors away, rural hospitals have too few patients to stay afloat financially, and virtual medicine isn't saving them. Virtual health care, in theory, sounds perfectly suited to the needs of rural populations. It kicks down the barrier of traveling great distances for medical needs and works increasingly well for diagnosing and managing the chronic and non-emergency health issues endemic to these parts of the country, such as diabetes, hypertension, asthma, and melanoma Yet success at implementing these virtual systems has been a patchwork. Unreliable access to at-home technology, broadband internet service, and cell reception have plagued some places, while ever present financial hurdles abound. Rather than usher in a long-anticipated telemedicine revolution in remote areas, COVID-19 has exposed its limitations, and highlighted what tools and regulations rural hospitals will need to survive the pandemic. read this insightful piece at https://www.nationalgeographic.com/science/2020/06/why-rural-hospitals-may-not-survive-coronavirus-telemedicine/
|