There are many reasons to be excited by the science being presented at this year’s American Society for Clinical Oncology meeting. The data...
Via Krishan Maggon
Get Started for FREE
Sign up with Facebook Sign up with X
I don't have a Facebook or a X account



 Your new post is loading...
Your new post is loading... Your new post is loading...
Your new post is loading...
There are many reasons to be excited by the science being presented at this year’s American Society for Clinical Oncology meeting. The data... Via Krishan Maggon 
No comment yet.
Sign up to comment
From
www

Abstract Via Krishan Maggon

Krishan Maggon 's curator insight,
May 10, 2015 1:55 PM
PNAS Emanuela Romano, doi: 10.1073/pnas.1417320112Ipilimumab-dependent cell-mediated cytotoxicity of regulatory T cells ex vivo by nonclassical monocytes in melanoma patientsEmanuela Romanoa,b,c,1, Monika Kusio-Kobialkab, Periklis G. Foukasc,d, Petra Baumgaertnerc,Christiane Meyerc, Pierluigi Ballabenie, Olivier Michielina,c, Benjamin Weidef, Pedro Romeroc, andDaniel E. Speiserc Author Affiliations Edited by Ira Mellman, Genentech, Inc., South San Francisco, CA, and approved March 30, 2015 (received for review September 9, 2014)
Krishan Maggon 's curator insight,
May 12, 2015 3:05 AM
PNAS Emanuela Romano, doi: 10.1073/pnas.1417320112
Ipilimumab-dependent cell-mediated cytotoxicity of regulatory T cells ex vivo by nonclassical monocytes in melanoma patientsEmanuela Romanoa,b,c,1, Monika Kusio-Kobialkab, Periklis G. Foukasc,d, Petra Baumgaertnerc,Christiane Meyerc, Pierluigi Ballabenie, Olivier Michielina,c, Benjamin Weidef, Pedro Romeroc, andDaniel E. Speiserc Author Affiliations Edited by Ira Mellman, Genentech, Inc., South San Francisco, CA, and approved March 30, 2015 (received for review September 9, 2014)
Monoclonal antibodies (mAbs) have inaugurated the concepts of tumor-targeted therapy and personalized medicine. A new family of mAbs is currently emerging in the clinic, which target immune cells rather than cancer cells. These immune-targeted therapies have recently demonstrated long-term tumor responses in adults with refractory/relapsing metastatic solid tumors. Pediatric cancers are different from their adult counterparts in terms of histological features and immune infiltrates. However, the same immune checkpoint targets can be expressed within the microenvironment of pediatric tumors. The benefits of immune checkpoint blockade in pediatric cancers are currently under evaluation in early phase clinical trials. Pediatr Blood Cancer © 2015 Wiley Periodicals, Inc. Via Krishan Maggon
Krishan Maggon 's curator insight,
March 30, 2015 1:02 AM
Tumor-targeted and immune-targeted monoclonal antibodies: Going from passive to active immunotherapyAurélien Marabelle MD, PhD1,2 andJuliet Gray MBBS, PhD3,*
Article first published online: 21 MAR 2015 DOI: 10.1002/pbc.25508 © 2015 Wiley Periodicals, Inc. Issue Pediatric Blood & CancerEarly View (Online Version of Record published before inclusion in an issue)

Via Krishan Maggon
Krishan Maggon 's curator insight,
March 3, 2015 12:18 PM
George K. Philips and Michael AtkinsTherapeutic uses of anti-PD-1 and anti-PD-L1 antibodies
Int. Immunol. (2015) 27 (1): 39-46 doi:10.1093/intimm/dxu095
Abstract
The concept of immunotherapy as a modality to treat cancer was recognized more than a hundred years ago. High-dose interleukin-2 (IL-2) was one of the first agents to demonstrate that the host's immune system can be harnessed to treat even advanced malignancy, as was shown in a subset of patients with renal cancer and melanoma. Many tumours are immunogenic and provoke a host immune response, but this is normally not sufficient to overcome host tolerance. For decades now, researchers have tried various methods to enhance host immunological responses, such as the use of non-specific immunotherapeutic cytokines, tumour vaccines, adoptive immunotherapy and the use of monoclonal antibodies against a wide variety of molecules. This review discusses the principles of the various types of immune therapy and focuses on some of the recent developments and successes in treatment. The article concentrates on the applications of immunotherapy in solid tumours, though it has immense value in haematological cancers. Via Krishan Maggon
Krishan Maggon 's curator insight,
February 19, 2015 3:58 AM
Surgery (Oxford)
Available online 14 February 2015 In Press, Corrected Proof — Note to users Cancer treatment Principles of cancer treatment by immunotherapyJenny Fernando, Satish Kumar doi:10.1016/j.mpsur.2015.01.004Get rights and content
A new tool for predicting how #NSCLC patients might respond to #immunotherapy paper by Kurt Schalper et al @JNCI_Now http://t.co/QqWmYZUa67
A Yale-led team of researchers has developed a new assay, or investigative tool, to measure the anti-tumor immune activity in non-small cell lung cancer tumors that could lead to a more accurate determination of which patients will respond to immune therapy drugs. Findings from the study were published in the Journal of the National Cancer Institute.
The assay simultaneously measures subpopulations of tumor-infiltrating lymphocytes (TILs), a type of white blood cell that attacks tumors. The presence of high amounts of TILs in tumors is associated with better treatment outcomes. The new method differs from existing immune-measuring assays in that it is objective, quantitative, and reproducible, said the paper’s first author, Dr. Kurt Schalper, associate research scientist in Yale School of Medicine and director of the Translational Immuno-oncology Laboratory at Yale Cancer Center. Via Krishan Maggon
#endcancer
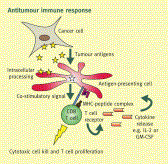
Abstract Cancer immunotherapy has proven to be challenging as it depends on overcoming multiple mechanisms that mediate immune tolerance to self-antigens. A growing understanding of immune tolerance has been the foundation for new approaches to cancer immunotherapy. Adoptive transfer of immune effectors such as antitumor mAb and chimeric antigen receptor T cells bypasses many of the mechanisms involved in immune tolerance by allowing for expansion of tumor-specific effectors ex vivo. Vaccination with whole tumor cells, protein, peptide, or dendritic cells has proven challenging, yet may be more useful when combined with other cancer immunotherapeutic strategies. Immunomodulatory approaches to cancer immunotherapy include treatment with agents that enhance and maintain T-cell activation. Recent advances in the use of checkpoint blockade to block negative signals and to maintain the antitumor response are particularly exciting. With our growing knowledge of immune tolerance and ways to overcome it, combination treatments are being developed, tested, and have particular promise. One example is in situimmunization that is designed to break tolerance within the tumor microenvironment. Progress in all these areas is continuing based on clear evidence that cancer immunotherapy designed to overcome immune tolerance can be useful for a growing number of patients with cancer. Cancer Res; 75(1); 5–10. ©2014 AACR. Via Krishan Maggon
Krishan Maggon 's curator insight,
January 7, 2015 11:32 AM
Published OnlineFirst December 18, 2014; doi: 10.1158/0008-5472. CAN-14-2538 Cancer Res January 1, 2015 75; 5Cancer Immunotherapy and Breaking Immune Tolerance: New Approaches to an Old ChallengeAmani Makkouk1 and George J. Weiner1,2,* +Author Affiliations 1Interdisciplinary Graduate Program in Immunology, University of Iowa, Iowa City, Iowa.2Holden Comprehensive Cancer Center and Department of Internal Medicine, University of Iowa, Iowa City, Iowa.↵*Corresponding Author:
I recently asked folks for their favorite hot targets in the tumor microenvironment space. Via Krishan Maggon
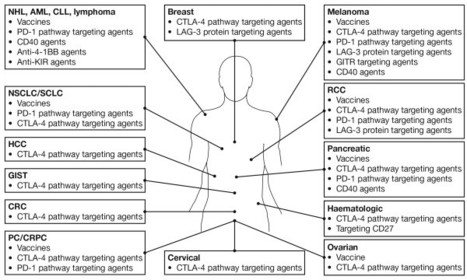
Until recently, most immunotherapeutic approaches used to fight cancer were ineffective, counteracted by the tumour’s ability to evade immune attack. However, extensive research has improved our understanding of tumour immunology and enabled the development of novel treatments that can harness the patient’s immune system and prevent immune escape. Over the last few years, through numerous clinical trials and real-world experience, we have accumulated a large amount of evidence regarding the potential for long-term survival with immunotherapy agents in various types of malignancy. The results of these studies have also highlighted a number of recurring observations with immuno-oncology agents, including their potential for clinical application across a broad patient population and for both conventional and unconventional response patterns. Furthermore, given the numerous immune checkpoints that exist and the multiple mechanisms used by tumours to escape the immune system, targeting distinct checkpoint pathways using combination approaches is an attractive therapeutic strategy with the potential to further enhance the antitumour immune response.
Fig 1. Immuno-oncology agentsa in clinical development across multiple tumour types.aSelected therapies and tumour types are shown: additional agents are, for example in phase 1 studies in patients with solid tumours [12]. AML, acute myeloid leukemia; CLL, chronic lymphocytic leukaemia; CRC, colorectal cancer; CRPC, castration-resistant prostate cancer; CTLA-4, cytotoxic T-lymphocyte antigen-4; GIST, gastrointestinal stromal tumour; HCC, hepatic cell carcinoma; LAG-3, lymphocyte activation gene 3; mAb, monoclonal antibody; NHL, non-Hodgkin lymphoma; NSCLC, non-small cell lung cancer; PC, prostate cancer; PD1, programmed death 1; RCC, renal cell carcinoma; SCLC, small cell lung cancer.
Ascierto and Marincola Journal of Translational Medicine 2014 12:141 doi:10.1186/1479-5876-12-141 Via Krishan Maggon
Krishan Maggon 's curator insight,
October 4, 2014 3:48 PM
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. What have we learned from cancer immunotherapy in the last 3 years? Paolo A Ascierto1* and Francesco M Marincola2 *Corresponding author: Paolo A Ascierto paolo.ascierto@gmail.com Author Affiliations 1Unit of Melanoma, Cancer Immunotherapy and Innovative Therapy Unit, Istituto Nazionale Tumori Fondazione “G. Pascale”, Via Mariano Semmola, 80131 Naples, Italy 2Sidra Medical and Research Centre, Doha, Qatar For all author emails, please log on. Journal of Translational Medicine 2014, 12:141 doi:10.1186/1479-5876-12-141 The electronic version of this article is the complete one and can be found online at:http://www.translational-medicine.com/content/12/1/141 Received:16 April 2014Accepted:13 May 2014Published:21 May 2014 © 2014 Ascierto and Marincola; licensee BioMed Central Ltd.
From
lbio
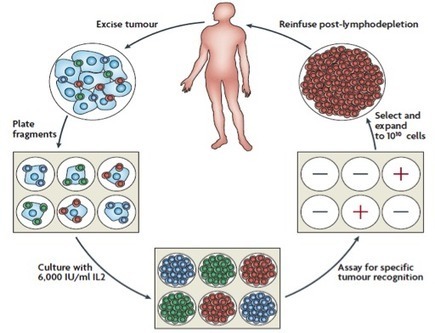
TIL Technology In the early stages of cancer, special immune cells known as tumor infiltrating lymphocytes (TILs) migrate to the tumor and launch an attack. However, this effect is usually short-lived because cancer adapts to evade immune detection and suppress immune response. Lion’s TIL technology is designed to overcome the immunosuppressive effects of cancer, while leveraging and enhancing the power of TILs to treat, and potentially cure, all solid tumors. Our TIL technology has demonstrated robust efficacy in Phase 2 clinical trials, indicating objective response rates of 49% in Stage 4 metastatic melanoma. Based on an adoptive cell therapy regimen developed by Steven A. Rosenberg, MD, chief of surgery at National Cancer Institute (NCI), it is currently in use as a physician-sponsored investigational treatment for Stage IV metastatic melanoma at NCI, MD Anderson Cancer Center, and the H. Lee Moffitt Cancer & Research Institute. Via Krishan Maggon
Gilbert C FAURE's insight:
TIL back on stage? they are not in memories of most students
Krishan Maggon 's curator insight,
July 23, 2014 10:13 PM
Lion Biotech TIL is in Phase II trials in advanced metastatic melanoma and in Phase I trials in combination with BRAF inhibitor Zelboraf (vemurafenib, Roche) and in another Phase I with Yervoy (Ipilimumab, BMS). all trials are with NCI. |
Via Krishan Maggon
Krishan Maggon 's curator insight,
May 15, 2015 4:02 AM
doi:10.1016/j.clinthera.2015.02.018
Clinical Therapeutics Volume 37, Issue 4, 1 April 2015, Pages 764–782 Review Article The Next Immune-Checkpoint Inhibitors: PD-1/PD-L1 Blockade in MelanomaKathleen M. Mahoney, MD, PhD1, 2, , , Gordon J. Freeman, PhD2, David F. McDermott, MD1

This review discusses the development of targeted and immune therapies for advanced melanoma, reviews current patient management, and highlights future directions. Via Krishan Maggon
Krishan Maggon 's curator insight,
April 25, 2015 3:37 AM
Review | April 23, 2015Therapeutic Advances and Treatment Options in Metastatic Melanoma FREE ONLINE FIRSTDouglas B. Johnson, MD, MSCI1,2; Jeffrey A. Sosman, MD1,2[+] Author AffiliationsJAMA Oncol. Published online April 23, 2015. doi:10.1001/jamaoncol.2015.0565
Via Krishan Maggon
Krishan Maggon 's curator insight,
March 9, 2015 3:56 AM
Highlights
• Melanoma treatment has been transformed using T-cell checkpoint antibodies. • Antibodies to CTLA-4 and PD-1 have had the largest impact on melanoma management. • Combination T-cell checkpoint therapy holds great promise for clinical development. • OX40 and 4-1BB are T cell costimulators with clinical potential in melanoma.

James P. Allison, who saw the devastating effects of cancer on his family, discovered a way to disable one of its main defenses. It was breakthrough of the year in Science two years ago Via Krishan Maggon
Via Krishan Maggon
Krishan Maggon 's curator insight,
February 10, 2015 2:37 AM
PS-Targeting Antibodies Block Tumor Suppression of Immune System Allowing Development of Robust Immune Responses Resulting in Statistically Significant Improvement in Anti-Tumor Activity; Specific Effects Seen in Decreased Levels of MDSCs and Other Immunosuppressive Lymphocytes and Increases in Tumor Fighting Immune Cells

#endcancer Via Krishan Maggon
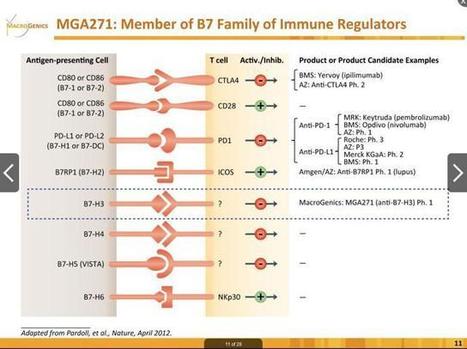
Checkpoint inhibitors are a big deal. What started with ipilimumab has now grown into a class of drugs which are being pursued vigorously by nearly every major pharmaceutical company in the world. In this crowded space, it's worth noting that B7-H3 is only being pursued by one company, MacroGenics (NASDAQ:MGNX). Via Krishan Maggon
Since cancer immunotherapy was declared the Breakthrough of the Year in 2013 by Science magazine the field has been on fire, and its relatively few experts have been on the run– explaining the nascent technology and related data to oncologists at... Via Krishan Maggon
Gilbert C FAURE's insight:
The overall message is clear: cancer immunotherapy is here to stay. It’s effective, and it’s sexy: as Jedd Wolchok, M.D., Ph.D., of the Memorial Sloan Kettering Cancer Center, said at ASCO, “We treat the patient. It’s the patient that treats the tumor.”

The BJC is owned by Cancer Research UK, a charity dedicated to understanding the causes, prevention and treatment of cancer and to making sure that the best new treatments reach patients in the clinic as quickly as possible.
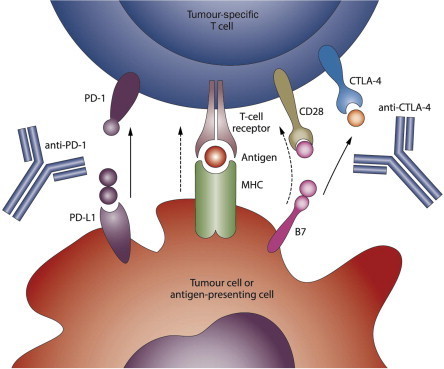
Fig 1. Targets of antibody immune modulators (Page et al, 2014)
background: Immune modulation in cancer refers to a range of treatments aimed at harnessing a patient’s immune system to achieve tumour control, stabilisation, and potential eradication of disease. A novel therapeutic drug class called immune checkpoint-blocking antibodies modulate T-cell pathways that regulate T cells and have the potential to reinvigorate an antitumour immune response. Ipilimumab was the first FDA-approved immune checkpoint antibody licensed for the treatment of metastatic melanoma (MM) and blocks a checkpoint molecule called cytotoxic T-lymphocyte antigen 4 (CTLA-4). methods: Herein we review the preclinical and clinical development of ipilimumab. We outline the mode of action of these agents and other immune checkpoint inhibitors, the management of their toxicities, and how to adequately assess response to treatment. results: As a result of these data, a number of other antibodies that block novel checkpoint molecules including programmed death-1 (PD-1), and corresponding ligands such as programmed death ligand-1 (PD-L1) are under preclinical and clinical development, and have demonstrated activity in multiple tumour types. conclusions: This review will summarise the mechanism of action and clinical development of immune checkpoint antibodies, as well as lessons learned in the management and assessment of patients receiving these agents. Via Krishan Maggon
Krishan Maggon 's curator insight,
October 2, 2014 11:02 AM
open access
Minireview British Journal of Cancer advance online publication 11 September 2014; doi: 10.1038/bjc.2014.348 Immune modulation for cancer therapy J Naidoo1, D B Page1 and J D Wolchok2,3 1Medical Oncology Fellow, Department of Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USA2Lloyd J. Old Chair of Clinical Investigation, Service Chief Melanoma and Immunotherapy Service, Associate Professor of Medicine, Department of Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USA3Ludwig Center for Cancer Immunotherapy, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USA Correspondence: Dr J Naidoo, E-mail: naidooj@mskcc.org Received 3 March 2014; Revised 20 May 2014; Accepted 23 May 2014
|