 Your new post is loading...
Your new post is loading...

|
Scooped by
nrip
|
While the US debates the value of the modality, a South Korean survey finds that patients like to use audio-only telehealth platforms to connect with their care provider - but their providers aren’t so sure. While telehealth is not legally allowed in South Korea, the Ministry of Health and Welfare temporarily permitted its use due to hospital closures at the start of the pandemic. Between February 24 and March 7, 2020, 6,840 patients used audio-based telehealth. Researchers sent surveys to patients and providers alike to gauge their satisfaction with the telehealth platform, which includes landline telephones and online services without video. They asked questions about ease-of-use, interaction quality, reliability, satisfaction, and future use. Around 87 % of patients reported that they were satisfied with their provider interaction and felt they could effectively express their feelings during an audio-only telehealth visit. Most patients (87.1 %) also responded that their telehealth visit was just as reliable as an in-person visit would have been. Meanwhile, the providers’ opinions differed drastically. Less than 10 % of doctors and nurses were satisfied with their ability to interact with patients through an audio-only telehealth visit compared to in-person visits (7.3 % and 9 %, respectively). Only 14 % of providers felt that the visits were as reliable as an in-person visit. Patients and providers also had differing opinions on the convenience of telehealth. Nearly 80 % of patients were satisfied with the convenience of telehealth and found it easy to use. Providers were not as satisfied, with only 38.2 % of doctors and 30 percent of nurses reporting that they found telehealth convenient. Overall, providers felt the negatives outweighed the positives for audio-only telehealth. While 85.8 % of the doctors and nurses agreed that telehealth is appropriate for emergency situations such as a pandemic, only 27.7 said it would be appropriate at all times. In contrast, 40 % of the doctors and nurses surveyed said telehealth would be appropriate if it involved an audio-visual platform, saying it would be easier to fully examine and diagnose a patient’s condition. read more at https://mhealthintelligence.com/news/audio-only-telehealth-has-its-fans-patients-and-its-critics-providers
|
|
Scooped by
nrip
|
“ATMAN AI”, an Artificial Intelligence algorithm that can detect the presence of COVID-19 disease in Chest X Rays, has been developed to combat COVID fatalities involving lung. ATMAN AI is used for chest X-ray screening as a triaging tool in Covid-19 diagnosis, a method for rapid identification and assessment of lung involvement. This is a joint effort of the DRDO Centre for Artificial Intelligence and Robotics (CAIR), 5C Network & HCG Academics. This will be utilized by online diagnostic startup 5C Network with support of HCG Academics across India. Triaging COVID suspect patients using X Ray is fast, cost effective and efficient. It can be a very useful tool especially in smaller towns in India owing to lack of easy access to CT scans there. This will also reduce the existing burden on radiologists and make CT machines which are being used for COVID be used for other diseases and illness owing to overload for CT scans. The novel feature namely “Believable AI” along with existing ResNet models have improved the accuracy of the software and being a machine learning tool, the accuracy will improve continually. Chest X-Rays of RT-PCR positive hospitalized patients in various stages of disease involvement were retrospectively analysed using Deep Learning & Convolutional Neural Network models by an indigenously developed deep learning application by CAIR-DRDO for COVID -19 screening using digital chest X-Rays. The algorithm showed an accuracy of 96.73%. read more at http://indiaai.gov.in/news/drdo-cair-5g-network-and-hcg-academics-develop-atman-ai
|
|
Scooped by
nrip
|
mRNA is a type of genetic material that tells your body how to make proteins. The two mRNA vaccines for SARS-CoV-2, the coronavirus that causes COVID-19, deliver fragments of this mRNA into your cells. The world’s first mRNA vaccines — the COVID-19 vaccines from Pfizer/BioNTech and Moderna — have made it in record time from the laboratory, through successful clinical trials, regulatory approval and into people’s arms. The high efficiency of protection against severe disease, the safety seen in clinical trials and the speed with which the vaccines were designed are set to transform how we develop vaccines in the future. We have two mRNA COVID-19 vaccines so far. But what else can this technology do? Once researchers have set up the mRNA manufacturing technology, they can potentially produce mRNA against any target. Manufacturing mRNA vaccines also does not need living cells, making them easier to produce than some other vaccines. So mRNA vaccines could potentially be used to prevent a range of diseases, not just COVID-19. Flu vaccine Moderna is already turning its attention to an mRNA vaccine against seasonal influenza. This would target the four seasonal strains of the virus the WHO predicts will be circulating. But the holy grail is a universal flu vaccine. This would protect against all strains of the virus (not just what the WHO predicts) and so wouldn’t need to be updated each year. The same researchers who pioneered mRNA vaccines are also working on a universal flu vaccine. Malaria vaccine There is no vaccine for Malaria. However, US researchers working with pharmaceutical company GSK have filed a patent for an mRNA vaccine against malaria. The mRNA in the vaccine codes for a parasite protein called PMIF. By teaching our bodies to target this protein, the aim is to train the immune system to eradicate the parasite. This malaria mRNA vaccine is an example of a self-amplifying mRNA vaccine. This means very small amounts of mRNA need to be made, packaged and delivered, as the mRNA will make more copies of itself once inside our cells. This is the next generation of mRNA vaccines after the “standard” mRNA vaccines seen so far against COVID-19. Cancer vaccines We already have vaccines that prevent infection with viruses that cause cancer. For example, hepatitis B vaccine prevents some types of liver cancer and the human papillomavirus (HPV) vaccine prevents cervical cancer. But the flexibility of mRNA vaccines lets us think more broadly about tackling cancers not caused by viruses. Some types of tumours have antigens or proteins not found in normal cells. If we could train our immune systems to identify these tumour-associated antigens then our immune cells could kill the cancer. Cancer vaccines can be targeted to specific combinations of these antigens. BioNTech is developing one such mRNA vaccine that shows promise for people with advanced melanoma. CureVac has developed one for a specific type of lung cancer, with results from early clinical trials. Then there’s the promise of personalised anti-cancer mRNA vaccines. If we could design an individualised vaccine specific to each patient’s tumour then we could train their immune system to fight their own individual cancer. Several research groups and companies are working on this. read the unedited original article at https://theconversation.com/3-mrna-vaccines-researchers-are-working-on-that-arent-covid-157858
|
|
Scooped by
nrip
|
A model has been developed by researchers at Indian Institute of Technology ,Kharagpur predicting alteration in metabolic reaction rates of lung cells post SARS-CoV-2 infection.
"We have used the gene expression of normal human bronchial cells infected with SARS-CoV-2 along with the macromolecular make-up of the virus to create this integrated genome-scale metabolic model. The growth rate predicted by the model showed a very high agreement with experimentally and clinically reported effects of SARS-CoV-2," said Dr Amit Ghosh, Assistant Professor, School of Energy Science and Engineering, IIT Kharagpur who coauthored the paper The research would lead to a better understanding of metabolic reprogramming and aid the development of better therapeutics to deal with viral pandemics, Summary: Metabolic flux analysis in disease biology is opening up new avenues for therapeutic interventions. Numerous diseases lead to disturbance in the metabolic homeostasis and it is becoming increasingly important to be able to quantify the difference in interaction under normal and diseased condition. While genome-scale metabolic models have been used to study those differences, there are limited methods to probe into the differences in flux between these two conditions. Our method of conducting a differential flux analysis can be leveraged to find which reactions are altered between the diseased and normal state. We applied this to study the altered reactions in the case of SARS-CoV-2 infection. We further corroborated our results with other multi-omics studies and found significant agreement. read the paper at https://journals.plos.org/ploscompbiol/article?id=10.1371/journal.pcbi.1008860
|
|
Scooped by
nrip
|
Vaccination Passports - What are they?
As mass vaccination programs are being rolled out globally, vaccine passports have become a major topic of discussion. COVID test results and proof of vaccine will be required in many countries for quarantine-free travel, just as it has been for polio and yellow fever vaccinations in the past. Countries will need to look at convenient and secure ways for verifying COVID-19 test results and vaccination information at airports and borders. The International Air Transport Association (IATA) has also called for a “global standard to securely record digital proof of vaccination”. They have been promoting the IATA Travel Pass Initiative (https://www.iata.org/en/programs/passenger/travel-pass/) In February, Qantas completed a trial run of an app for this purpose on an international repatriation flight from Frankfurt to Darwin. The idea behind the app is that health or border officials and airline staff may be able to easily verify COVID-19 test results and vaccination history of an individual. The app links customers with certified testing labs to allow their results to be automatically uploaded onto it. Similar digital solutions are being developed in several other countries around the world to enable travel again. For instance, travellers from Singapore will receive a notarized certificate following a negative COVID-19 test that they can present at airports around the world. Another example is France taking part in a month-long trial of a vaccine passport that leverages a smart phone app. Its important that such digital health technologies, whether apps or chip cards, or health tracker add ons, be easy to use. It important that the process be as seamless as possible for flyers share the relevant information as well as get the information validated by the ground and air staff so they people can travel internationally, again, safely! image source: https://foto.wuestenigel.com/person-hands-holding-a-covid-19-passport/ image license: https://creativecommons.org/licenses/by/2.0/
|
|
Scooped by
nrip
|
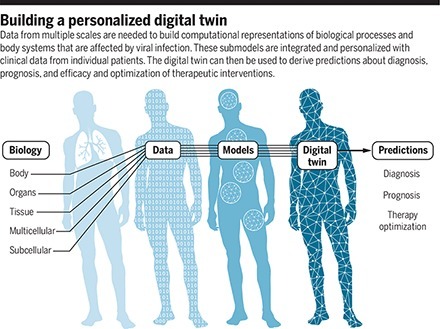
No current tool can predict the course of disease and help a doctor decide on the most appropriate treatment for an individual COVID-19 patient. Digital twins are software replicas of the dynamic function and failure of engineered products and processes. The medical analog, patient-specific digital twins, could integrate known human physiology and immunology with real-time patient-specific clinical data to produce predictive computer simulations of viral infection and immune response. Such medical digital twins could be a powerful addition to our arsenal of tools to fight future pandemics, combining mechanistic knowledge, observational data, medical histories, and the power of artificial intelligence (AI). Although medical digital twins are much more difficult to develop than those for engineered devices, they have begun to find applications in improving human health. Examples include the “artificial pancreas” for type 1 diabetes patients Building a personalized digital twin Data from multiple scales are needed to build computational representations of biological processes and body systems that are affected by viral infection. These submodels are integrated and personalized with clinical data from individual patients. The digital twin can then be used to derive predictions about diagnosis, prognosis, and efficacy and optimization of therapeutic interventions. Digital twins describing infection and treatment require the development, validation, and integration of numerous component submodels in the context of a rapidly developing scientific understanding of biological behaviors and continual generation of new experimental and clinical data. Although individual laboratories may construct submodels, the development of comprehensive digital twins will require laboratories and research groups around the world to integrate and validate submodels independently, with only limited central coordination. Enabling such parallel development requires a flexible simulation architecture that uses a multiscale map of all the relevant components of a patient's response to viral infection, as well as responses to available treatments. read the paper at https://science.sciencemag.org/content/371/6534/1105.full
|
|
Scooped by
nrip
|
With cases soaring across the globe, the Covid-19 pandemic is nowhere near its end, but with three vaccines reporting trial data and two apparently nearing approval by the US FDA, it may be reaching a pivot point. In what feels like a moment of drawing breath and taking stock, international researchers are turning their attention from the present back to the start of the pandemic, aiming to untangle its origin and asking what lessons can be learned to keep this from happening again. Two efforts are happening in parallel. On November 5, the World Health Organization quietly published the rules of engagement for a long-planned and months-delayed mission that creates a multinational team of researchers who will pursue how the virus leaped species. Meanwhile, last week, a commission created by The Lancet and headed by the economist and policy expert Jeffrey Sachs announced the formation of its own international effort, a task force of 12 experts from nine countries who will undertake similar tasks. Both groups will face the same complex problems. It has been approximately a year since the first cases of a pneumonia of unknown origin appeared in Wuhan, China, and about 11 months since the pneumonia’s cause was identified as a novel coronavirus, probably originating in bats. The experts will have to retrace a chain of transmission—one or multiple leaps of the virus from the animal world into humans—using interviews, stored biological samples, lab assays, environmental surveys, genomic data, and the thousands of papers published since the pandemic began, all while following a trail that may have gone cold. The point is not to look for patient zero, the first person infected—or even a hypothetical bat zero, the single animal from which the novel virus jumped. It’s likely neither of those will ever be found. The goal instead is to elucidate the ecosystem—physical, but also viral—in which the spillover happened and ask what could make it likely to happen again. more at WIRED : https://www.wired.com/story/two-global-efforts-try-to-trace-the-origin-of-the-covid-virus/?utm_source=pocket-newtab-intl-en
|
|
Scooped by
nrip
|
We are directionally headed towards a significant shift in the way care is delivered. The rapid up scaling of virtual care capacity and the mainstreaming of Telehealth have given rise to new digital health tools. Self-triaging and contact tracing for COVID-19 infection detection are among the new breed of digital health applications that startups to big firms alike were looking at to seize the emerging opportunities. Telehealth is here to stay. Healthcare is shifting to virtual care models. Digital front door apps are all the rage. What else is emerging that could change the way we experience care? While telehealth is now the de facto mode of accessing healthcare for most low-acuity and routine care needs, a number of related technology-led trends are quietly gaining ground as well. Here the author looks at a few of these and opinionates on their potential impact on healthcare consumer experiences. "contactless" experiences: Covid has made us all afraid to touch any surface exposed to the public. Nowhere is this fear more prominent than a hospital or clinic setting. Healthcare executives now speak of airport check-in type of experiences for healthcare appointments, both for in-person and virtual visits. Technology-enabled workflows now enable patients to complete most of the registration formalities prior to the visit, be it a virtual consult or a clinic visit. Registration kiosks in hospital lobbies may soon be enabled with facial recognition software to eliminate the need for touching any surface. Routine examinations are also going virtual, with many diagnostic procedures now possible through remotely controlled devices. Caregivers are beginning to do their patient rounds through virtual visits. This trend will only grow in the coming years. Contact tracing Inspired by the success of India, Singapore and South Korea, contact tracing applications on Bluetooth-enabled devices have been positioned as an effective means to track and trace infections to reduce the spread of COVID-19 Despite many setbacks, contact tracing's potential for deployment within communities and populations for uses beyond COVID-19 has longer-term potential, and this could be the single most important technology-enabled healthcare program to come out of the COVID-19 crisis. Remote monitoring and automated communication Healthcare executives are more motivated than ever to keep their populations healthy in their homes. A vast and growing array of automated communication tools allows caregivers to use rule-based messaging to push everything from health coaching, post-discharge care instructions, and appointment reminders through IVR, text, SMS, and mobile alerts. Data mining tools can identify subsets of populations at risk and enable caregivers to intervene on time. A New York-based COVID-19 Rapid Response Coalition involving tech giant Amazon that targeted high-risk populations through SMS campaigns that reached up to 10,000 members a day, is an example of how automated communication tools can serve populations in a crisis and during normal times. The use of digital health and automated communication tools has also improved healthcare outcomes by reducing no-shows for appointments, increased adherence to medication regimens, and targeted interventions during adverse events. There is an unprecedented opportunity today to use telehealth technologies in the complete continuum of care. However, healthcare enterprises and their technology partners need to make them more user-friendly. That will determine success for new technology-enabled virtual care models. Every health system has to design the digital experience that is suited for their patient populations while remembering to address the needs of caregivers who will deliver and manage the experiences.
|
|
|
Scooped by
nrip
|
We developed and validated an accurate in-hospital mortality prediction score in a live EHR for automatic and continuous calculation using a novel model that improved upon SOFA. The COVID-19 pandemic created an emergent need for a novel, accurate, and location and context-sensitive EHR-computable tool to predict mortality in hospitalized patients with and without COVID-19. Because developing a new score can take years, a predictive model must rely on well-validated scores. In contrast, COVID-19 is a novel disease for which existing scores may be of limited but unknown predictive value. As such, a predictive framework relying on multiple previously validated scores that can incorporate new information but only keeps the new inputs that explicitly improve performance is required. Stacked generalization provides a solution. A stacked model is built upon one or more baseline model(s) (e.g. SOFA) and incorporates additional models only when they improve prediction. Materials and Methods We developed, verified, and deployed a stacked generalization model to predict mortality using data available in the EHR by combining five previously validated scores and additional novel variables reported to be associated with COVID-19-specific mortality. We verified the model with prospectively collected data from 12 hospitals in Colorado between March 2020 and July 2020. We compared the area under the receiver operator curve (AUROC) for the new model to the SOFA score and the Charlson Comorbidity Index. Results The prospective cohort included 27,296 encounters, of which 1,358 (5.0%) were positive for SARS-CoV-2, 4,494 (16.5%) required intensive care unit care, 1,480 (5.4%) required mechanical ventilation, and 717 (2.6%) ended in death. The Charlson Comorbidity Index and SOFA scores predicted mortality with an AUROC of 0.72 and 0.90, respectively. Our novel score predicted mortality with AUROC 0.94. In the subset of patients with COVID-19, the stacked model predicted mortality with AUROC 0.90, whereas SOFA had AUROC of 0.85. Discussion Stacked regression allows a flexible, updatable, live-implementable, ethically defensible predictive analytics tool for decision support that begins with validated models and includes only novel information that improves prediction. read the paper abstract at https://academic.oup.com/jamia/advance-article/doi/10.1093/jamia/ocab100/6273353 read the entire paper at https://academic.oup.com/jamia/advance-article-pdf/doi/10.1093/jamia/ocab100/37905236/ocab100.pdf
|
|
Scooped by
nrip
|
Since the start of the pandemic, new technologies have been developed to help reduce the spread of the infection. Some of the most common safety measures today include measuring a person’s temperature, covering your nose and mouth with a mask, contact tracing, disinfection, and social distancing. Many businesses have adopted various technologies, including those with artificial intelligence (AI) underneath, helping to adhere to the COVID-19 safety measures. As an example, numerous airlines, hotels, subways, shopping malls, and other institutions are already using thermal cameras to measure an individual’s temperature before people are allowed entry. In its turn, public transport in France relies on AI-based surveillance cameras to monitor whether or not people are social-distancing or wearing masks. Another example is requiring the download of contact-tracing apps delivered by governments across the globe. However, there are a number of issues. While many of these solutions help to ensure that COVID-19 prevention practices are observed, many of them have flaws or limits. In this article, we will cover some of the issues creating obstacles for fighting the pandemic. Issue #1. Manual temperature scanning is tricky Issue #2. Monitoring crowds is even more complex Issue #3. Contact tracing leads to privacy concerns Issue #4. UV rays harm eyes and skin Issue #5. UVC robots are extremely expensive Issue #6. No integration, no compliance, no transparency Regardless of the safety measures in place and existing issues, innovations are already playing a vital role in the fight against COVID-19. By improving on existing technology, we can make everyone safer as we all adjust to the new normal. read the details at https://www.altoros.com/blog/whats-wrong-with-ai-tools-and-devices-preventing-covid-19/
|
|
Scooped by
nrip
|
Two scientific leaps, in machine learning algorithms and powerful biological imaging and sequencing tools , are increasingly being combined to spur progress in understanding diseases and advance AI itself. Cutting-edge, machine-learning techniques are increasingly being adapted and applied to biological data, including for COVID-19. Recently, researchers reported using a new technique to figure out how genes are expressed in individual cells and how those cells interact in people who had died with Alzheimer's disease. Machine-learning algorithms can also be used to compare the expression of genes in cells infected with SARS-CoV-2 to cells treated with thousands of different drugs in order to try to computationally predict drugs that might inhibit the virus. While, Algorithmic results alone don't prove the drugs are potent enough to be clinically effective. But they can help identify future targets for antivirals or they could reveal a protein researchers didn't know was important for SARS-CoV-2, providing new insight on the biology of the virus read the original article which speaks about a lot more at https://www.axios.com/ai-machine-learning-biology-drug-development-b51d18f1-7487-400e-8e33-e6b72bd5cfad.html
|
|
Scooped by
nrip
|
There is a seriousness, almost an urgent kind, amongst the healthcare ecosystem to adopt digital technologies more openly as compared to the pre - covid era. Since we have always been talking about the importance of taking healthcare digital, this acceptance of digital technologies has impacted us tremendously and favourably. Plus91's Digital Health Systems have always been a few years too soon for the market, and Covid just fast-forwarded the world to use us right away. What is your take on virtual methods of providing treatment? All virtual treatment methods, whether it is TeleHealth, Remote Monitoring, Tele Pathology are very much a necessity. Covid has simply brought them into the limelight and forced the world to adopt them quickly. I believe they all benefit healthcare immensely, and thus should be adopted wholeheartedly by doctors and patients. They end up offering a wider variety of options for both and allow a far richer treatment mindset to get created in the coming years. Doctors benefit from being accessible to patients from across the globe more easily and frequently for both offering care as well as 2nd/3rd opinions. This helps them acquire experience on a wider range of patients besides the ones that come to them purely due to geographical viability. Patients benefit a lot as they can access doctors more easily, and also get doctors who may be in a different part of the world from them who are experts at dealing with a specific condition without having to bear the cost of travel. What impact do you want to create in the medical field? I want to make healthcare more holistic, error-free, and open. I believe in the distant future we will be able to address the whole issue of disease and mankind will be completely focused on health from the wellness perspective rather than a treatment perspective. And I want to be an integral part of that change. read the whole interview at : https://www.eatmy.news/2021/04/nrip-nihalani-i-want-to-make-healthcare.html
|
|
Scooped by
nrip
|
Cancer is next problem to tackle with mRNA tech, says BioNTech founder
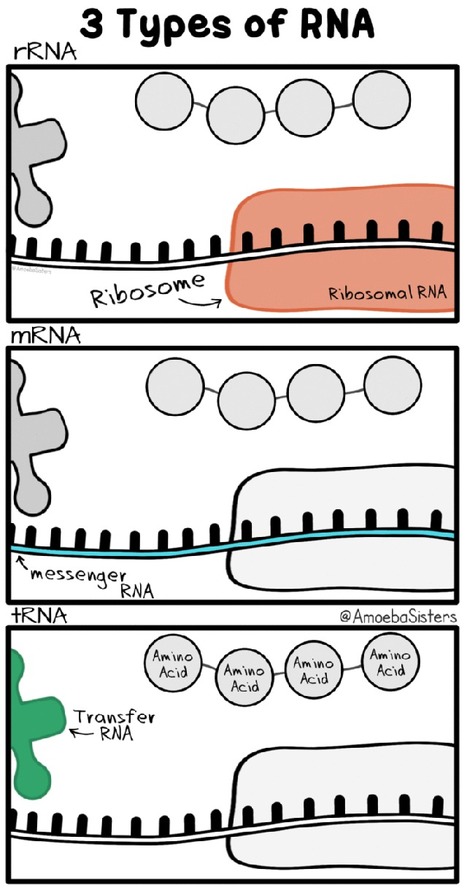
The co-founder of German company BioNTech, which successfully delivered the first widely distributed coronavirus vaccine, said that the mRNA technology it used will soon be put to work tackling cancer. Özlem Türeci, who started BioNTech alongside her husband, said that she had been working to use the body's immune system to combat cancer tumors before the coronavirus pandemic stopped the world. “We have several different cancer vaccines based on mRNA,” The coronavirus vaccine made by BioNTech(and also Pfizer) uses messenger RNA, or mRNA, to deliver instructions to the body to make proteins that will alert it to attack a certain virus. The same technology can in theory be used for cancer tumors. What is mRNA ? Messenger RNA (mRNA) is a single-stranded RNA molecule that is complementary to one of the DNA strands of a gene. The mRNA is an RNA version of the gene that leaves the cell nucleus and moves to the cytoplasm where proteins are made. During protein synthesis, an organelle called a ribosome moves along the mRNA, reads its base sequence, and uses the genetic code to translate each three-base triplet, or codon, into its corresponding amino acid.
The mRNA Approach to Vaccines
mRNA vaccines are a new type of vaccine to protect against infectious diseases. To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, they teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies. mRNA vaccines have been studied before for flu, Zika, rabies, and cytomegalovirus (CMV). As soon as the necessary information about the virus that causes COVID-19 was available, scientists began designing the mRNA instructions for cells to build the unique spike protein into an mRNA vaccine. Future mRNA vaccine technology may allow for one vaccine to provide protection for multiple diseases, thus decreasing the number of shots needed for protection against common vaccine-preventable diseases.
|
|
Scooped by
nrip
|
Mobile health (mhealth) tools delivered through wireless technology are emerging as effective strategies for - delivering quality training,
- ensuring rapid clinical decision making and
- monitoring implementation of simple and effective interventions in under-resourced settings.
Link to the paper updated - https://www.researchgate.net/publication/349807156_Introduction_of_Mobile_Health_Tools_to_Support_COVID-19_Training_and_Surveillance_in_Ogun_State_Nigeria We share our early experience of development and deployment of the InStrat COVID-19 health worker training application (App) based on the MediXcel Lite #mHealth platform by Plus91 technologies in Ogun state, Western Nigeria where the country's first case was reported. This App was designed to - directly provide frontline health workers with accurate and up-to-date information about COVID-19;
- enable them to quickly identify, screen and manage COVID-19 suspects;
- provide guidance on specimen collection techniques and safety measures to observe within wards and quarantine centres dealing with COVID-19.
The App was deployed in 271 primary health care facilities in Ogun State and a total of 311 health workers were trained. Of the 123 health workers who completed knowledge pre-and post-tests, their average test score improved from 47.5(±9.4) % to 73.1(±10.0) %, P < 0.0001 after using the tutorial. Rapid adoption and uptake were driven largely by public-private sector involvement as well as certification with reported satisfaction levels of over 95%. Challenges encountered included a lack of universal availability of android phones for frontline health workers, lack of internet access in remote areas and a need to incentivize the workers. The timely deployment of this App targeting primary health care workers, mostly in hard-to-reach areas, obviated the need for conventional didactic training with potential of savings in training costs and time and could be applied to similar contexts. This novel use of mobile health training to shore up training of front line health workers in a resource-limited setting during a pandemic has applicability to similar contexts.
|
|
Scooped by
nrip
|
As healthcare providers battle an increasing influx of patients and dwindling inventory – including critical personal protective equipment (PPE) supplies like masks, ventilators, and hospital beds – they are relying more heavily on their digital tools and applications than ever before. Prior to this recent pandemic, research shows that 84 percent of people have experienced problems with digital services in the last year. In the middle of a global health crisis, there’s no tolerance for bad performance when it’s a matter of a patients’ health. To improve these experiences, health IT professionals must leverage AI and machine learning to pinpoint the moment digital issues arise and automatically remediate issues. This saves IT teams time and resources that could be spent creating new services that will further improve the patient and doctor’s experience during the crisis. Digital strategies that HealthIT leaders must consider to support healthcare professionals regardless of where and when they are providing care. - Real-time analytics and monitoring
- Remote monitoring
Read the entire article at https://hitconsultant.net/2020/05/20/digital-strategies-healthit-must-prioritize-during-covid-19/#.Xvhd1JMzZPt
|
|
Scooped by
nrip
|
With fear of COVID-19 keeping many routine visitors away, rural hospitals have too few patients to stay afloat financially, and virtual medicine isn't saving them. Virtual health care, in theory, sounds perfectly suited to the needs of rural populations. It kicks down the barrier of traveling great distances for medical needs and works increasingly well for diagnosing and managing the chronic and non-emergency health issues endemic to these parts of the country, such as diabetes, hypertension, asthma, and melanoma Yet success at implementing these virtual systems has been a patchwork. Unreliable access to at-home technology, broadband internet service, and cell reception have plagued some places, while ever present financial hurdles abound. Rather than usher in a long-anticipated telemedicine revolution in remote areas, COVID-19 has exposed its limitations, and highlighted what tools and regulations rural hospitals will need to survive the pandemic. read this insightful piece at https://www.nationalgeographic.com/science/2020/06/why-rural-hospitals-may-not-survive-coronavirus-telemedicine/
|



























The idea of being able to literally have a check-up has jumped to the forefront in terms of convenience. While some believe Audio-only is a level of impersonal (providers), most whom needed to use the service (patients) believed it was very effect in terms of being diagnosed. Practitioners of the medical arts feel that this innovative idea can be expanded for a more accurate interaction with patients by also integrating visual/video with this program. With the rapid expansion of tech, it may not be long before you only need to actually go to the hospital when in need of critical care. This would lead to hospitals being able to take in more patients that actually need to be there vs ones taking up space because of the "convenience" of being closer physically. The one drawback I foresee may be the fact of availability of your actual doctor, though it could be be supplemented by other professionals in the field.