mRNA is a type of genetic material that tells your body how to make proteins. The two mRNA vaccines for SARS-CoV-2, the coronavirus that causes COVID-19, deliver fragments of this mRNA into your cells.
The world’s first mRNA vaccines — the COVID-19 vaccines from Pfizer/BioNTech and Moderna — have made it in record time from the laboratory, through successful clinical trials, regulatory approval and into people’s arms.
The high efficiency of protection against severe disease, the safety seen in clinical trials and the speed with which the vaccines were designed are set to transform how we develop vaccines in the future.
We have two mRNA COVID-19 vaccines so far. But what else can this technology do?
Once researchers have set up the mRNA manufacturing technology, they can potentially produce mRNA against any target. Manufacturing mRNA vaccines also does not need living cells, making them easier to produce than some other vaccines.
So mRNA vaccines could potentially be used to prevent a range of diseases, not just COVID-19.
Flu vaccine
Moderna is already turning its attention to an mRNA vaccine against seasonal influenza. This would target the four seasonal strains of the virus the WHO predicts will be circulating.
But the holy grail is a universal flu vaccine. This would protect against all strains of the virus (not just what the WHO predicts) and so wouldn’t need to be updated each year.
The same researchers who pioneered mRNA vaccines are also working on a universal flu vaccine.
Malaria vaccine
There is no vaccine for Malaria. However, US researchers working with pharmaceutical company GSK have filed a patent for an mRNA vaccine against malaria.
The mRNA in the vaccine codes for a parasite protein called PMIF. By teaching our bodies to target this protein, the aim is to train the immune system to eradicate the parasite.
This malaria mRNA vaccine is an example of a self-amplifying mRNA vaccine. This means very small amounts of mRNA need to be made, packaged and delivered, as the mRNA will make more copies of itself once inside our cells. This is the next generation of mRNA vaccines after the “standard” mRNA vaccines seen so far against COVID-19.
Cancer vaccines
We already have vaccines that prevent infection with viruses that cause cancer. For example, hepatitis B vaccine prevents some types of liver cancer and the human papillomavirus (HPV) vaccine prevents cervical cancer.
But the flexibility of mRNA vaccines lets us think more broadly about tackling cancers not caused by viruses.
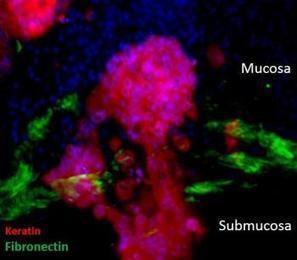
Some types of tumours have antigens or proteins not found in normal cells. If we could train our immune systems to identify these tumour-associated antigens then our immune cells could kill the cancer.
Cancer vaccines can be targeted to specific combinations of these antigens. BioNTech is developing one such mRNA vaccine that shows promise for people with advanced melanoma. CureVac has developed one for a specific type of lung cancer, with results from early clinical trials.
Then there’s the promise of personalised anti-cancer mRNA vaccines. If we could design an individualised vaccine specific to each patient’s tumour then we could train their immune system to fight their own individual cancer. Several research groups and companies are working on this.
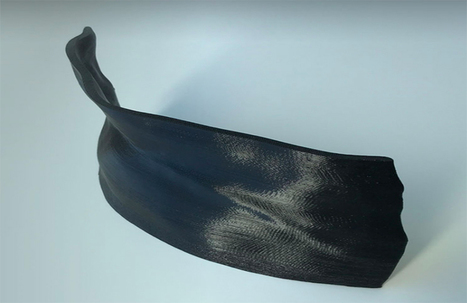
Adaptiiv Medical Technologies said that the U.S. military will use its 3D bolus software to treat American veterans with cancer at Walter Reed National Military Medical Center.
Adaptiiv designed its software to convert patient CT scan data into a digital model that can be used to print a bolus that conforms to patient anatomy, according to the company. The structure is then exported as an STL file that can be printed in a matter of hours on a healthcare facility’s existing 3D printer or on a printer provided by the company.
Using Adaptiiv software, practitioners can 3D print patient-specific, uniform thickness boluses, modulated boluses for modulated electron radiation therapy (MERT), high-dose-rate (HDR) surface brachytherapy and other potential ancillary devices. The boluses are printed using durable, tissue-equivalent materials that hold their shape and do not degrade during treatments. Patients typically use the same 3D printed bolus for the duration of their treatment, reducing the risk of infection. Patients are more comfortable throughout the treatment period, while set-up and production times are reduced, the company said
The military is utilizing 3D bolus for cancer treatments of veterans at Walter Reed National Military Medical Center.
Adaptiiv is the first company in the world to receive FDA 510k clearance for 3D printing software used in radiation oncology. The company’s software is used in the United States, Canada, Australia, Israel, Ireland, Hong Kong and England.
Personalized medicine is hoping to reach new heights thanks to the Cancer Moonshot, but won't get off the ground without a community-wide commitment to sharing big data.
The precision medicine community has long since recognized that sharing big data, including clinical records, genomic sequencing data, community-level health indicators, and research results, will be critical to making progress against cancer, neurodegenerative diseases, inherited conditions, and expensive chronic diseases like diabetes.
“Why is data sharing important? Because cancer is complex,” said Kenneth C. Anderson, MD, President-elect of the American Society of Hematology (ASH). Anderson specializes in multiple myeloma, a blood cancer with treatment options that hinge on the genetic variances of each and every patient.
“We’re learning so much about cancer, and applying these insights to drug development has been incredibly fruitful,” he continued. “Now we have treatments that are specifically targeted to patients’ genetic mutations. Not only are these treatments more effective — because they correct a specific mutation — they also minimize harmful side effects that we see with traditional total-body anticancer medicines.”
However, the continued development of these treatments cannot be sustained without a commitment to data sharing, he added.
In 2011, a 52-year-old runner and yoga enthusiast walked into the office of Monica Loghin, a neuro-oncologist at MD Anderson Cancer Center in Houston, complaining of numbness and weakness in her lower limbs and difficulty controlling her bladder.
The symptoms were of grave concern, as the patient had previously undergone surgery for breast cancer that had spread to her brain. If such a cancer returns post-surgery, that is often a sign the patient doesn’t have much time left.
An MRI confirmed that the breast cancer had again spread to the woman’s cerebrospinal fluid. Loghin ordered testing of that fluid to see if the patient might have certain biomarkers that could be targeted by existing drugs. (A biomarker is a DNA sequence or protein associated with the disease; different biomarkers can suggest specific treatments, depending on the disease and other factors.) She asked for tests that could detect tumor cells circulating in the blood.
The cancer cells in the fluid bathing the woman’s spinal cord and brain chambers did, in fact, have a lot of the protein that controls a glucose (sugar) transporter that drives cancer cells. The cancer cells in the fluid also had a lot of HER2, a protein associated with aggressive breast cancers but also treatable with a drug called Herceptin (trastuzumab). The drug is usually taken intravenously, but Loghin had heard of a couple of cases in which Herceptin was delivered directly into the cerebrospinal fluid via a flexible tube, or catheter. The patient agreed to this experimental treatment.
It took only a week for the news to improve. After the first infusion of Herceptin, the patient’s cancer numbers were down. Within a few weeks, her cancer cell numbers had fallen so low that her immune system had begun to take over, clearing out the remaining cancer cells. Nearly two and a half years later, the patient is still alive and well enough to do yoga. Another MD Anderson patient who had a similar disease profile and therapy is also alive and well one year after treatment.
This case outlines the dream of personalized medicine: A disease is analyzed at the molecular level. The analysis identifies a drug target. The drug gets delivered where it needs to go. The patient gets better. And while this hopeful scenario has yet to become commonplace, it is becoming more and more the norm for many breast cancer patients.
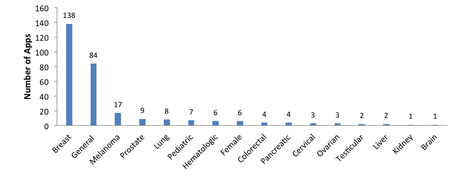
Which apps can be used by chronic cancer patients to help them with their illness and overall health?
There are literally thousands of medical apps in the marketplace and it is very difficult to sift through them and find out which ones are easy to use, practical and helpful.
Joan Justice did some research, asked some patients, and read a lot of reviews to try and get an idea of which ones were helpful for chronic cancer patients and published this...
It includes some of my recommendations: ClinicalTrialsSeek and Pillboxie along with many others...
Since the beginning of the 21st century, mobile phones have become nearly ubiquitous. At the end of 2011, there were an estimated 6 billion mobile subscriptions, accounting for approximately 87% of the global population
Rapid technological convergence has led to the emergence of smartphones—feature-rich phones that combine the voice and text messaging functions of basic phones with powerful computing technology that can support third-party applications, sensing, Internet access, and wireless connectivity with other devices.
According to a 2012 report from the Pew Internet and American Life Project, 85% of US adults own a cell phone of some kind and 53% own a smartphone
The combination of their popularity, technical capabilities, and proximity to their owners makes them an attractive platform for the delivery of health promotion and disease management interventions
Systematic review methodology, as described by Moher et al , was used to guide the collection and characterization of eligible apps from the official smartphone stores and the evidence on app utility or effectiveness from the health literature. We developed a systematic search strategy that attempted to identify all relevant apps and studies and we provide a systematic presentation and synthesis of the characteristics of the apps and the studies.
RESULTS:
The search of the mobile phone market yielded 1314 potentially relevant apps, of which 309 apps met our selection criteria (Figure 1); 90.3% (279/309) of apps were available on the iPhone or Android markets . Twelve apps were available on more than one platform (10 were available in two stores and 2 in three stores). Therefore, there were a total of 295 unique apps.
Release date information was available for only 38.0% (112/295) of the apps from Apple, Android, and BlackBerry, as the remainder had produced updated versions and only published their date of update. Release date information was not available for apps on the Nokia market.
Half of the apps (50.2%, 148/295) were free to download. Of those free-to-download apps, 8 were trial versions of the full pay-for-download applications. These free apps offered limited versions of the full apps, restricting access to the full suite of features.
The majority of the apps did not describe their organizational affiliation (64.1%, 189/295). Of those that provided organizational information, 63.2% (67/106) were affiliated with a non-profit, 26.4% (28/106) with a commercial company (eg, Health Monitor Network), 9.4% (10/106) with a university or medical institution, and 1 app was affiliated with a government institution (eg, National Institutes for Health).
Apps affiliated with not-for-profit organizations (non-profit, university, medical institution, or government) were more likely to be free (?21=16.3, P<.001). Apps that did not disclose their affiliation were more likely to have a price (?21=50.1, P<.001).
Every year IBM makes predictions about 5 technology innovations that stand to change the way we live within the next 5 years.
This year, one of those 5 is Personalized Cancer Treatment.
In five years, doctors will routinely use your DNA to keep you well. Cancer will be treated on a DNA level in both the patient and tumor, at a scale and speed never before possible.
Researchers uncover new ties between genetics and skin cancer by mining patients’ medical records.
Usually, studying the relationship between DNA and disease involves comparing the genomes of thousands of people with a disorder to the genomes of thousands of people who don’t. These studies can be expensive and may take years, requiring researchers to identify patients, enroll them in the study, and collect the genomic data.
A more cost-effective and speedier alternative is to mine the growing pool of genetic data in electronic medical records as reported by researchers in Nature Biotechnology.
These records chronicle a patient’s health care history, which can include physician’s notes, lab test results, and the billing codes hospitals submit to health insurance companies to receive payments.
The idea behind the new method for genetic discover is to be able to “reuse” the data in these records for medical discoveries, says Joshua Denny, a physician-scientist at Vanderbilt University School of Medicine.
To identify previously unknown relationships between disease and DNA variants, Denny and colleagues grouped around 15,000 billing codes from medical records into 1,600 disease categories. Then, the researchers looked for associations between disease categories and DNA data available in each record.
Their biggest new findings all involved skin diseases (just a coincidence, says Josh Denny, the lead author): non melanoma skin cancer and two forms of skin growths called keratosis, one of which is pre-cancerous. The team was able to validate the connection between these conditions and their associated gene variants in other patient data.
The co-founder of German company BioNTech, which successfully delivered the first widely distributed coronavirus vaccine, said that the mRNA technology it used will soon be put to work tackling cancer.
Özlem Türeci, who started BioNTech alongside her husband, said that she had been working to use the body's immune system to combat cancer tumors before the coronavirus pandemic stopped the world.
“We have several different cancer vaccines based on mRNA,”
The coronavirus vaccine made by BioNTech(and also Pfizer) uses messenger RNA, or mRNA, to deliver instructions to the body to make proteins that will alert it to attack a certain virus. The same technology can in theory be used for cancer tumors.
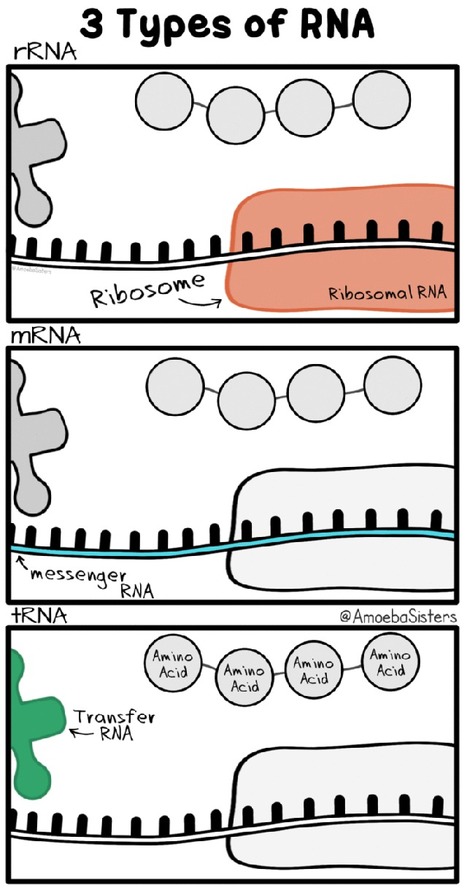
What is mRNA ?
Messenger RNA (mRNA) is a single-stranded RNA molecule that is complementary to one of the DNA strands of a gene. The mRNA is an RNA version of the gene that leaves the cell nucleus and moves to the cytoplasm where proteins are made. During protein synthesis, an organelle called a ribosome moves along the mRNA, reads its base sequence, and uses the genetic code to translate each three-base triplet, or codon, into its corresponding amino acid.
The mRNA Approach to Vaccines
mRNA vaccines are a new type of vaccine to protect against infectious diseases. To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, they teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.
mRNA vaccines have been studied before for flu, Zika, rabies, and cytomegalovirus (CMV). As soon as the necessary information about the virus that causes COVID-19 was available, scientists began designing the mRNA instructions for cells to build the unique spike protein into an mRNA vaccine.
Future mRNA vaccine technology may allow for one vaccine to provide protection for multiple diseases, thus decreasing the number of shots needed for protection against common vaccine-preventable diseases.
Deep mind will use data available to it via a new partnership with Jikei University Hospital in Japan to refine its artificially intelligent (AI) breast cancer detection algorithms.
Google AI subsidiary DeepMind has partnered with Jikei University Hospital in Japan to analyze mammagrophy scans from 30,000 women.
DeepMind is furthering its cancer research efforts with a newly announced partnership.
The London-based Google subsidiary said it has been given access to mammograms from roughly 30,000 women that were taken at Jikei University Hospital in Tokyo, Japan between 2007 and 2018.
Deep mind will use that data to refine its artificially intelligent (AI) breast cancer detection algorithms.
Over the course of the next five years, DeepMind researchers will review the 30,000 images, along with 3,500 images from magnetic resonance imaging (MRI) scans and historical mammograms provided by the U.K.’s Optimam (an image database of over 80,000 scans extracted from the NHS’ National Breast Screening System), to investigate whether its AI systems can accurately spot signs of cancerous tissue.
Healthcare data is increasingly being analyzed and complex algorithms created to help various aspects of the healthcare ecosystem.
A big problem is the availability of huge data sets, and where available, the prevention of their misuse. Its great that Deepmind is able to source data sets , (being a sub of Google, am sure plays a role), and hopefully they will put their deep mind ;) to good use and be able to improve detection algorithms.
I have written previously on this, and it will be useful for patients and if the data sets do help create both faster as well as more accurate detection algorithms in the future.
Faulty genes are major triggers and drivers of cancer, and the more knowledge we have about them individually, the better we can predict, track, and treat the disease in a way that is specific to individual patients' particular genetic promoters. To do this, researchers need models that are as realistic as possible.Cell and animal models help, but they do not meet the need at the tissue level. Now, using tissue engineering techniques, researchers have created a human colon model that allows them to identify and track the genes that drive colorectal cancer from initial abnormal mass to invasive tumor.
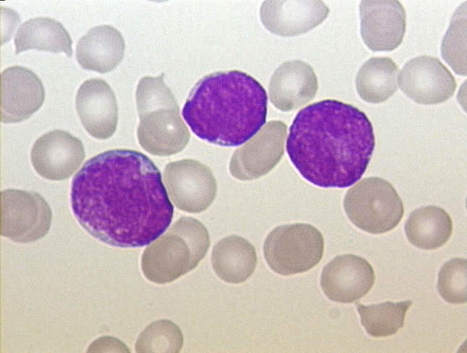
A University of Pennsylvania-developed personalized immunotherapy has been awarded the U.S. Food and Drug Administration’s Breakthrough Therapy designation for the treatment of relapsed and refractory adult and pediatric acute lymphoblastic leukemia (ALL). The investigational therapy, known as CTL019, is the first personalized cellular therapy for the treatment of cancer to receive this important classification.
In early-stage clinical trials at the Hospital of the University of Pennsylvania and the Children’s Hospital of Philadelphia, 89% of ALL patients who were not responding to conventional therapies went into complete remission after receiving CTL019.
The investigational treatment pioneered by the Penn team begins by removing patients' T cells via an apheresis process similar to blood donation, then genetically reprogramming them in Penn’s Clinical Cell and Vaccine Production Facility. After being infused back into patients’ bodies, these newly built “hunter” cells both multiply and attack, targeting tumor cells that express a protein called CD19. Tests reveal that the army of hunter cells can grow to more than 10,000 new cells for each single engineered cell patients receive.
“If you’re dealing with a disease like cancer that can be arrived at by multiple pathways, it makes sense that you’re not going to find that each patient has taken the same path” - John McDonald, a professor in the School of Biology at the Georgia Institute of Technology in Atlanta.
If a driver is traveling to New York City, I-95 might be their route of choice. But they could also take I-78, I-87 or any number of alternate routes. Most cancers begin similarly, with many possible routes to the same disease. A new study found evidence that assessing the route to cancer on a case-by-case basis might make more sense than basing a patient’s cancer treatment on commonly disrupted genes and pathways.
The study found little or no overlap in the most prominent genetic malfunction associated with each individual patient’s disease compared to malfunctions shared among the group of cancer patients as a whole. “This paper argues for the importance of personalized medicine, where we treat each person by looking for the etiology of the disease in patients individually,” said McDonald,
“The findings have ramifications on how we might best optimize cancer treatments as we enter the era of targeted gene therapy.”
The research was published February 11 online in the journal PANCREAS and was funded by the Georgia Tech Foundation and the St. Joseph’s Mercy Foundation.
In the study, researchers collected cancer and normal tissue samples from four patients with pancreatic cancer and also analyzed data from eight other pancreatic cancer patients that had been previously reported in the scientific literature by a separate research group.
McDonald’s team compiled a list of the most aberrantly expressed genes in the cancer tissues isolated from these patients relative to adjacent normal pancreatic tissue.
The study found that collectively 287 genes displayed significant differences in expression in the cancers vs normal tissues. Twenty-two cellular pathways were enriched in cancer samples, with more than half related to the body’s immune response. The researchers ran statistical analyses to determine if the genes most significantly abnormally expressed on an individual patient basis were the same as those identified as most abnormally expressed across the entire group of patients.
The researchers found that the molecular profile of each individual cancer patient was unique in terms of the most significantly disrupted genes and pathways.
“If you’re dealing with a disease like cancer that can be arrived at by multiple pathways, it makes sense that you’re not going to find that each patient has taken the same path” - John McDonald, a professor in the School of Biology at the Georgia Institute of Technology in Atlanta.
Cancer research is something I'm particularly interested in and would try to go into someday and I found this interesting because it shows how medicine has evolved and becoming more personalized.
Personalized medicine is the art and science of “coupling established clinical–pathological indexes with state-of-the-art molecular profiling to create diagnostic, prognostic and therapeutic strategies precisely tailored to each patient’s requirements.”1
The clinical development and regulatory approval of targeted agents that have therapeutic benefit in molecularly defined patient subsets has highlighted the value of personalized medicine, which can be leveraged in clinical trials so that the identification of eligible patients for certain trials is optimized based on the patient’s molecular testing. These targeted patient groups are often rare and expensive to identify, particularly in the field of oncology, making clinical trials targeting these populations difficult to enroll.
Patient pre-profiling, determining a patient’s tumor-specific molecular profile, could have great value for physicians and patients as they consider potential clinical trial options. To the extent that a molecular profile is broad, encompassing many potential target alterations, one can easily imagine benefits such as more efficient enrollment, increased participation by physicians and patients and more informed treatment decisions. Pre-profiling before a trial is set up at a particular site offers a more efficient approach to enrollment while also providing greater molecular testing to support patient care.
Our current understanding of cancer biology indicates that cancer is a large number of niche diseases that may be targeted with therapies against specific molecular alterations. Drug development under this model creates new challenges for both the development program itself and for patient care. Patient preprofiling promises to leverage high throughput genomic profiling, bioinformatics and, where possible, new trial designs to drive better trial matching and faster enrollment to clinical trials.
Preprofiling may require new relationships and business models, most notably, among patients, clinical sites, biopharmaceutical sponsors and CROs to enable data sharing, site start-up and funding of the genomic testing. The adoption of a new model of patient genomic profiling linked to novel clinical trial designs testing targeted therapies in development is becoming a key response to the challenge to develop many compounds in niche populations in a cost and time sensitive manner.
La gestión de ensayos clínicos es complicada. En este caso, se añade la dificultad de dividir a los pacientes según sus mutaciones. A medida que la medicina personalizada avanza, se hace más necesaria una colaboración internacional entre centros u hospitales para abarcar a todos los pacientes posibles en los ensayos clínicos. Esto también hace necesario tener en cuenta las diferencias que puedan existir entre las leyes regulatorias de los ensayos clínicos de los distintos países.
Learn how doctors will be able to develop targeted cancer therapy based on you and your cancer’s genetics.
How to personalize cancer treatment
Once a doctor sequences your full genome as well as your cancer’s DNA, mapping that information to the right treatment is difficult. Today, these types of DNA-based plans, where available, can take weeks or even months. Cognitive systems will decrease these times, while increasing the availability by providing doctors with information they can use to quickly build a focused treatment plan in just days or even minutes – all via the cloud.
Within five years, deep insights based on DNA sequencing will be accessible to more doctors and patients to help tackle cancer. By using cognitive systems that continuously learn about cancer and the patients who have cancer, the level of care will only improve. No more assumptions about cancer location or type, or any disease with a DNA link, like heart disease and stroke.
New tools for analyzing genes are allowing doctors to personalize treatment for some lung cancer patients.
Imagine your doctor being able to scan your DNA from a biopsy and pinpoint the medicine that will work best for you. This type of high-tech approach is a clinical reality for advanced lung cancer at The Ohio State Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute (OSUCCC – James).
The technology, known as next generation "multiplex" gene sequencing, analyzes 50-plus genes in DNA extracted from a tumor biopsy for particular genetic mutations.
Previous technology required pathologists to analyze one mutation per tube in a sequencing reaction, but next-generation genome sequencing assesses more than 2,500 mutations in a single reaction.
Knowing which mutations are present in lung tumors can help doctors tailor a patient's treatment to the unique genetic features present in his or her cancer cells.
The knowledge can also help in the development of new drugs that target previously unrecognized gene mutations in lung tumors. I often compare these genes to the gas pedal in a car — when activated, these genes make the cancer grow. By breaking the linkage between the gas pedal and the motor (or interfering with these "driver" mutations) with specific targeted drugs, doctors can stop this growth and often make the cancer shrink.
That's especially important in lung cancer because the majority of patients with this disease are diagnosed in the later stages, meaning it's important to start effective therapies quickly.
For example, a patient could be given a standard chemotherapy and expect a 25- to 30- percent response rate/shrinkage of a tumor. But if the treatment team knows that a patient has a mutation in a gene called EGFR, we can offer him or her a pill (erlotinib and afatinib are approved for this use in the United States), which has a 75-percent response rate and fewer side effects.
Gene sequencing is now considered the standard of care for stage-4 lung cancer patients at The OSUCCC – James and a handful of other centers across the United States — and several clinical trials evaluating molecular targeted therapies for patients with stage-3 lung cancers will soon start at The OSUCCC – James.
Lung cancer remains the number one cause of cancer death in the United States, and in the world, among both men and women. More than 200,000 cases are diagnosed annually in the United States. Each year during the month of November, physicians and others observe lung cancer awareness month, which sheds light on this terrible disease.
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.



 Your new post is loading...
Your new post is loading...