ECHORD++ 's mission is to close the innovation gap between what is available on the market and the public sector's needs. The project has selected as its focus for the next five years the two areas of
Get Started for FREE
Sign up with Facebook Sign up with X
I don't have a Facebook or a X account



|
Scooped by
Sergio Ariño Blasco
onto Comprehensive Geriatric Assessment |
ECHORD++ 's mission is to close the innovation gap between what is available on the market and the public sector's needs. The project has selected as its focus for the next five years the two areas of

 Your new post is loading... Your new post is loading...
Background: Although calcium and vitamin D (CaD) supplementation may affect chronic disease in older women, evidence of long-term effects on health outcomes is limited. Objective: To evaluate long-term health outcomes among postmenopausal women in the Women’s Health Initiative CaD trial. Design: Post hoc analysis of long-term postintervention follow-up of the 7-year randomized intervention trial of CaD. (ClinicalTrials.gov: NCT00000611) Setting: A multicenter (n = 40) trial across the United States. Participants: 36 282 postmenopausal women with no history of breast or colorectal cancer. Intervention: Random 1:1 assignment to 1000 mg of calcium carbonate (400 mg of elemental calcium) with 400 IU of vitamin D3 daily or placebo. Measurements: Incidence of colorectal, invasive breast, and total cancer; disease-specific and all-cause mortality; total cardiovascular disease (CVD); and hip fracture by randomization assignment (through December 2020). Analyses were stratified on personal supplement use. Results: For women randomly assigned to CaD versus placebo, a 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years (1817 vs. 1943 deaths; hazard ratio [HR], 0.93 [95% CI, 0.87 to 0.99]), along with a 6% increase in CVD mortality (2621 vs. 2420 deaths; HR, 1.06 [CI, 1.01 to 1.12]). There was no overall effect on other measures, including all-cause mortality (7834 vs. 7748 deaths; HR, 1.00 [CI, 0.97 to 1.03]). Estimates for cancer incidence varied widely when stratified by whether participants reported supplement use before randomization, whereas estimates on mortality did not vary, except for CVD mortality. Limitation: Hip fracture and CVD outcomes were available on only a subset of participants, and effects of calcium versus vitamin D versus joint supplementation could not be disentangled. Conclusion: Calcium and vitamin D supplements seemed to reduce cancer mortality and increase CVD mortality after more than 20 years of follow-up among postmenopausal women, with no effect on all-cause mortality. Primary Funding Source: National Heart, Lung, and Blood Institute of the National Institutes of Health.

From
jamanetwork

People who were infected with SARS-CoV-2 tended to score slightly worse on cognitive assessments—particularly in memory, reasoning, and tasks that require executive function—than those who were not infected, according to data from about 113 000 participants in England. The score was th
From
jamanetwork
Variations in several biomarkers, including proteins found in cerebrospinal fluid (CSF), might appear 6 to 18 years before a person develops Alzheimer disease, according to a prospective cohort study that included more than 600 participants in China with no family history of the condition.

From
www
This podcast episode explores the fastest-growing neurologic condition in the world, Parkinson’s disease. What have we learned in recent years, and where are the greatest hopes for the future?
Cognitive changes in iRBD begin up to 10 years prior to phenoconversion, starting with a decline in executive function followed by attention, then memory and visuospatial dysfunction closer to time of phenoconversion
Sergio Ariño Blasco's insight:
Considerar polisomnografia en el diagnostico diferencial...
Admission cognition, ADL independence, and physical function predicted physical function change following post-hospitalization rehabilitation. Inverse findings for admission physical function and ADL independence predictors suggest independence with ADL is not necessarily aligned with mobility-related function. Findings highlight that functional recovery is multifactorial and requires comprehensive assessment throughout SNF rehabilitation.
Sergio Ariño Blasco's insight:
Obvio, probablemente los instrumentos utilizados tienen efecto techo-suelo y no discriminan cambios. Lástima que no se incorpore la situación funcional/cognitiva previa al ingreso

In the present study, the use of telemedicine in the management of nursing home residents requiring a call to the EMCC decreased the number of dispatches to the ED by 18%.
By reducing the number of dispatches to our ED, the implementation of telemedicine in nursing homes could prevent 450 unplanned admissions per year in our ED and 65,000 admissions per year in all French EDs. There are many benefits to be expected, both individually in terms of morbidity of older individuals by avoiding cognitive decline, iatrogenic complications, and other adverse events commonly associated with unplanned hospital admissions and collectively by limiting inappropriate hospitalizations and their associated costs.
Sergio Ariño Blasco's insight:
El dispositivo registraba...signos vitales, cámara para el registro de foto y video y la posibilidad de registro EKG. Reducción de hasta el 18% de las derivaciones a ucias.
Frailty measures derived from primary care electronic health records (EHRs) offer a rapid and inexpensive means of segmenting large populations of older people
Older patients are typically underrepresented in clinical trials despite representing a major proportion of the patient population. We aim to describe the feasibility of performing body composition measures, physical function measures, and patient-reported
“Common sense oncology is about focusing on outcomes that matter to patients. The field needs to generate better evidence, with less bias, and use ‘universal goals’ of older patients to guide decisions. The narrative of ‘newer is better’ or ‘do something’ needs scrutiny”
|
In their article, Ganguli and colleagues characterized a new measure of health care utilization—“health care contact days.” The editorialists find the measure a promising new way to understand ho
From
www
A vision for the future NHS workforce

From
jamanetwork
This review discusses diagnosis and first-line treatment options for dry mouth, oral candidiasis, and recurrent aphthous ulcers.
Team-based care models such as the Patient-Centered Medical Home are associated with improved patient health outcomes, better team coordination and collaboration, and increased well-being among health care professionals. Despite these attributes, hindrances to wider adoption remain. In addition, some health care professionals have sought to practice independent of the physician-led health care team, potentially undermining patient access to physicians who have the skills and training to deliver whole-person, comprehensive, and longitudinal care. In this paper, the American College of Physicians reaffirms the importance of the physician-led health care team and offers policy recommendations on professionalism, payment models, training, licensure, and research to support the expansion of dynamic clinical care teams.
Sergio Ariño Blasco's insight:
Reflexiones corporativistas (probablemente pertinentes en la actualidad) desde un modelo americano donde la existencia de Nurse Practitioners y Physician Assistants ya existen desde hace 50 años.
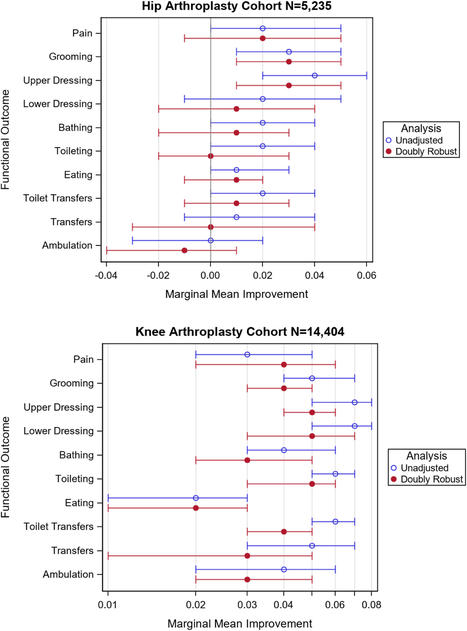
Evidence supports including home OT/PT in postoperative pain management guidelines more for TKA than THA. These findings may be attributable to different postoperative rehabilitation approaches for TKA and THA. For example, early TKA recovery focuses on remediating postoperative impairments. In comparison, patients with THA follow conservative precautions to reduce the 2.1% incidence of dislocation. 10 Therefore, compensatory techniques take precedence over remediation. During compensatory rehabilitation, a high OT/PT dose may have less impact due to temporary compensation through quick environmental modifications like shower chairs, grab bars, and patient education
The Centers for Medicare & Medicaid Services (CMS) Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents—Payment Reform enabled participating NFs to bill Medicare for providing on-site care to eligible long-stay residents meeting specified severity criteria due to any of 6 medical conditions, as an alternative to hospitalization. For billing purposes, residents were required to meet clinical criteria severe enough to warrant hospitalization.
Our findings lend support to the practice of treating residents for these 6 conditions on-site, when clinically appropriate, instead of transferring to a hospital. It is advisable that NF medical directors consider our findings and be reassured that treatment within the facility is often the better choice for residents and their health outcomes. Further research is warranted to develop best practice criteria to guide decisions as to when to treat residents with these conditions on-site vs in the hospital. In addition to outcomes measured in this study, there are other benefits to treating nursing facility residents on-site, such as supporting continuity of care and supporting residents to remain in a stable, familiar environment.
Sergio Ariño Blasco's insight:
Parece que funciona como era de prever, si bien la clave es que existe una transferencia de pago por episodio agudo a la residencia (difícil de trasladar este modelo a nuestro entorno).
IntroducciónDada la creciente adopción de la ecografía clínica en medicina,
From
www
Wearable Technologies in Cardiovascular Medicine This article reviews the use of digital wearable technologies for monitoring of three common cardiovascular conditions: hypertension, hear
The 10 steps are as follows: (1) select every variable that measures a health problem; (2) exclude variables with more than 5% missing values; (3) recode the responses to 0 (no deficit) through 1 (deficit); (4) exclude variables when coded deficits are too rare (< 1%) or too common (> 80%); (5) screen the variables for association with age; (6) screen the variables for correlation with each other; (7) count the variables retained; (8) calculate the frailty index scores; (9) test the characteristics of the frailty index; (10) use the frailty index in analyses. In our worked example, we created a 61-item frailty index following these 10 steps
|